

Tachyarrhythmias During Hospitalization for COVID-19 or Multisystem Inflammatory Syndrome in Children and Adolescents
- PMID: 36250670
- PMCID: PMC9673680
- DOI: 10.1161/JAHA.122.025915
Tachyarrhythmias During Hospitalization for COVID-19 or Multisystem Inflammatory Syndrome in Children and Adolescents
Abstract
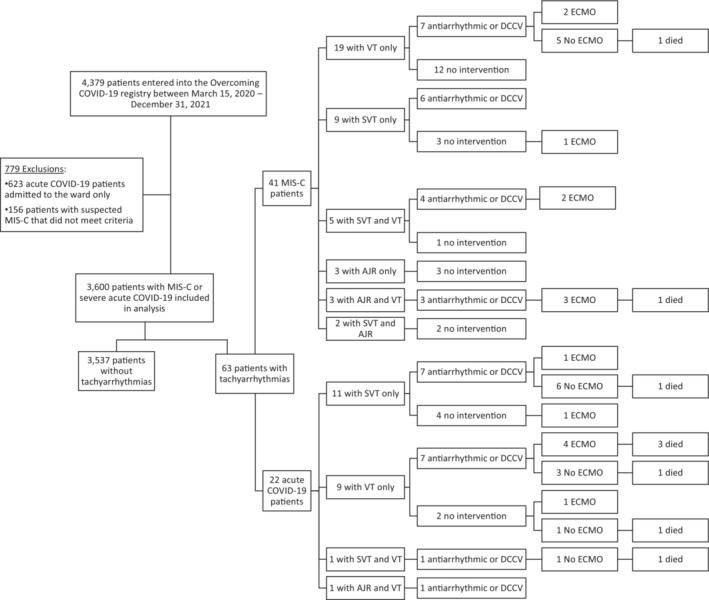
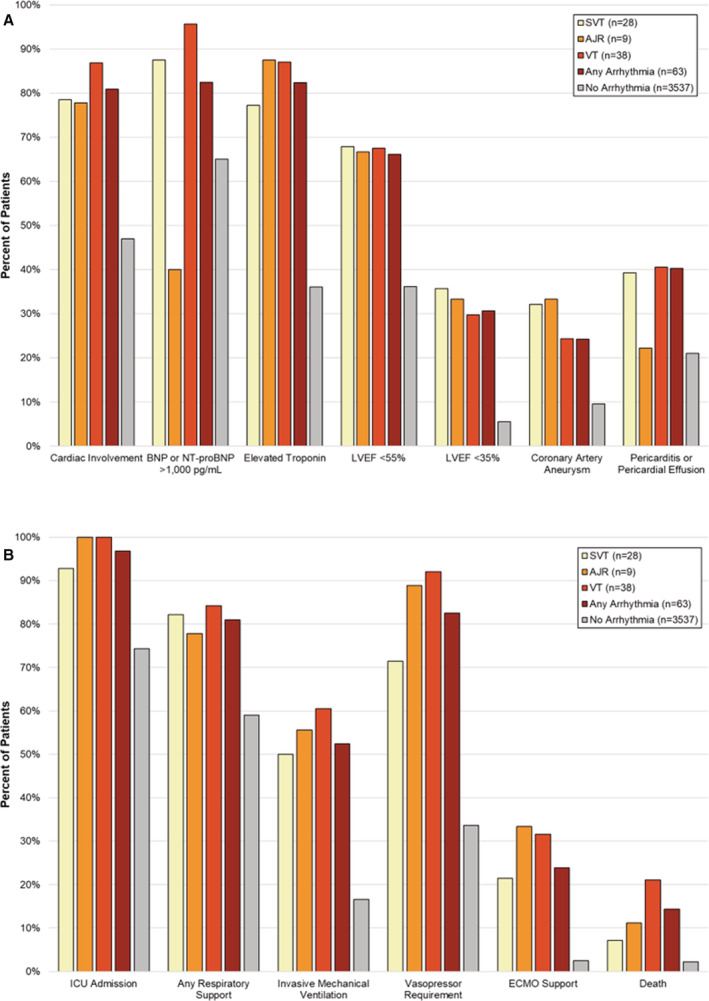
Background Cardiac complications related to COVID-19 in children and adolescents include ventricular dysfunction, myocarditis, coronary artery aneurysm, and bradyarrhythmias, but tachyarrhythmias are less understood. The goal of this study was to evaluate the frequency, characteristics, and outcomes of children and adolescents experiencing tachyarrhythmias while hospitalized for acute severe COVID-19 or multisystem inflammatory syndrome in children. Methods and Results This study involved a case series of 63 patients with tachyarrhythmias reported in a public health surveillance registry of patients aged <21 years hospitalized from March 15, 2020, to December 31, 2021, at 63 US hospitals. Patients with tachyarrhythmias were compared with patients with severe COVID-19-related complications without tachyarrhythmias. Tachyarrhythmias were reported in 22 of 1257 patients (1.8%) with acute COVID-19 and 41 of 2343 (1.7%) patients with multisystem inflammatory syndrome in children. They included supraventricular tachycardia in 28 (44%), accelerated junctional rhythm in 9 (14%), and ventricular tachycardia in 38 (60%); >1 type was reported in 12 (19%). Registry patients with versus without tachyarrhythmia were older (median age, 15.4 [range, 10.4-17.4] versus 10.0 [range, 5.4-14.8] years) and had higher illness severity on hospital admission. Intervention for treatment of tachyarrhythmia was required in 37 (59%) patients and included antiarrhythmic medication (n=31, 49%), electrical cardioversion (n=11, 17%), cardiopulmonary resuscitation (n=8, 13%), and extracorporeal membrane oxygenation (n=9, 14%). Patients with tachyarrhythmias had longer hospital length of stay than those who did not, and 9 (14%) versus 77 (2%) died. Conclusions Tachyarrhythmias were a rare complication of acute severe COVID-19 and multisystem inflammatory syndrome in children and adolescents and were associated with worse clinical outcomes, highlighting the importance of close monitoring, aggressive treatment, and postdischarge care.
Keywords: COVID‐19; multisystem inflammatory syndrome in children (MIS‐C); tachyarrhythmia.
Figures
References
-
- Feldstein LR, Tenforde MW, Friedman KG, Newhams M, Rose EB, Dapul H, Soma VL, Maddux AB, Mourani PM, Bowens C, et al. Characteristics and outcomes of US children and adolescents with multisystem inflammatory syndrome in children (MIS‐C) compared with severe acute COVID‐19. JAMA. 2021;325:1074–1087. doi: 10.1001/jama.2021.2091 - DOI - PMC - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
