

Longitudinal Evaluation of Biomarkers in Wound Fluids from Venous Leg Ulcers and Split-thickness Skin Graft Donor Site Wounds Treated with a Protease-modulating Wound Dressing
- PMID: 36250733
- PMCID: PMC9811302
- DOI: 10.2340/actadv.v102.325
Longitudinal Evaluation of Biomarkers in Wound Fluids from Venous Leg Ulcers and Split-thickness Skin Graft Donor Site Wounds Treated with a Protease-modulating Wound Dressing
Abstract
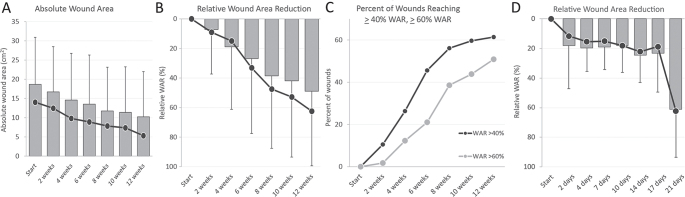
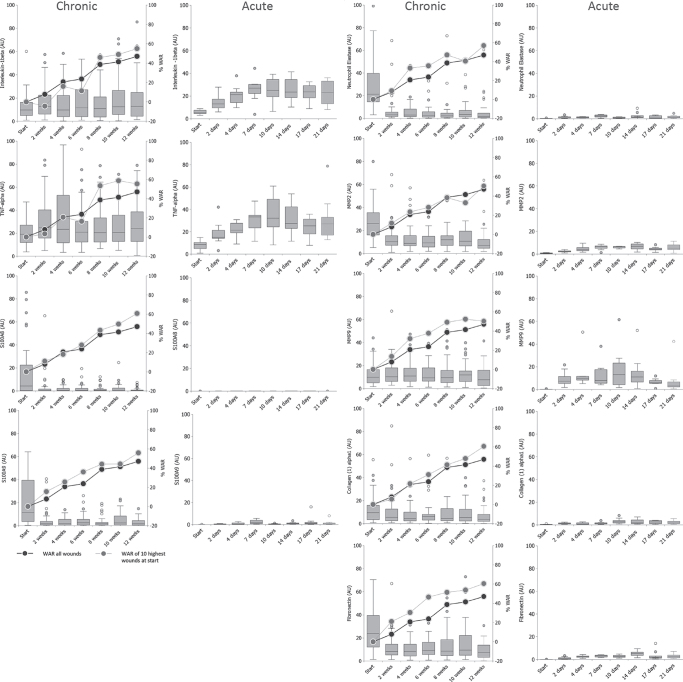
Venous leg ulcers represent a clinical challenge and impair the quality of life of patients. This study examines impaired wound healing in venous leg ulcers at the molecular level. Protein expression patterns for biomarkers were analysed in venous leg ulcer wound fluids from 57 patients treated with a protease-modulating polyacrylate wound dressing for 12 weeks, and compared with exudates from 10 acute split-thickness wounds. Wound healing improved in the venous leg ulcer wounds: 61.4% of the 57 patients with venous leg ulcer achieved a relative wound area reduction of ≥ 40%, and 50.9% of the total 57 patients achieved a relative wound area reduction of ≥ 60%. Within the first 14 days, abundances of S100A8, S100A9, neutrophil elastase, matrix metalloproteinase-2, and fibronectin in venous leg ulcer exudates decreased significantly and remained stable, yet higher than in acute wounds. Interleukin-1β, tumour necrosis factor alpha, and matrix metalloproteinase-9 abundance ranges were similar in venous leg ulcers and acute wound fluids. Collagen (I) α1 abundance was higher in venous leg ulcer wound fluids and was not significantly regulated. Overall, significant biomarker changes occurred in the first 14 days before a clinically robust healing response in the venous leg ulcer cohort.
Conflict of interest statement
Figures

References
-
- Marston WA, Ennis WJ, Lantis JC, Kirsner RS, Galiano RD, Vanscheidt W, et al. . Baseline factors affecting closure of venous leg ulcers. J Vasc Surg Venous Lymphat Disord 2017; 5: 829–835.e1. - PubMed
-
- Kantor J, Margolis DJ. A multicentre study of percentage change in venous leg ulcer area as a prognostic index of healing at 24 weeks. Br J Dermatol 2000; 142: 960–964. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
