

Exploratory study to assess feasibility of intracerebral hemorrhage detection by point of care cranial ultrasound
- PMID: 36251105
- PMCID: PMC9576831
- DOI: 10.1186/s13089-022-00289-z
Exploratory study to assess feasibility of intracerebral hemorrhage detection by point of care cranial ultrasound
Abstract
Background: Limited studies have evaluated the use of ultrasound for detection of intracerebral hemorrhage (ICH) using diagnostic ultrasound Transcranial Doppler machines in adults. The feasibility of ICH detection using Point of care Ultrasound (POCUS) machines has not been explored. We evaluated the feasibility of using cranial POCUS B mode imaging performed using intensive care unit (ICU) POCUS device for ICH detection with a secondary goal of mapping optimal imaging technique and brain topography likely to affect sensitivity and specificity of ICH detection with POCUS.
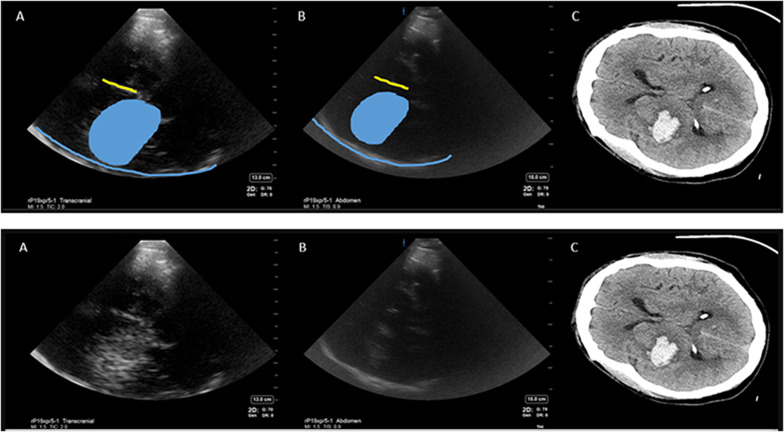
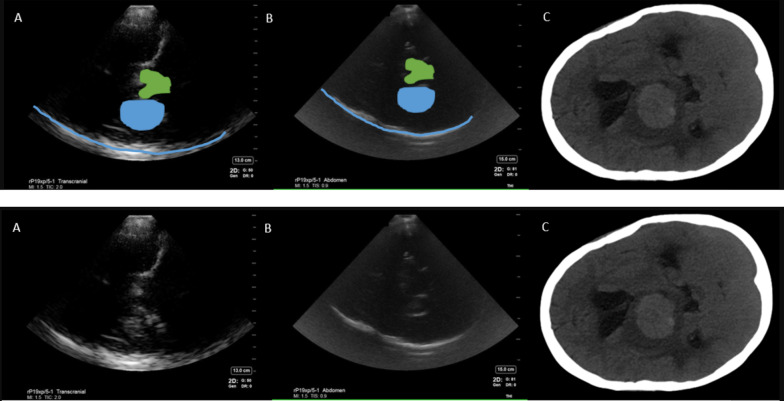
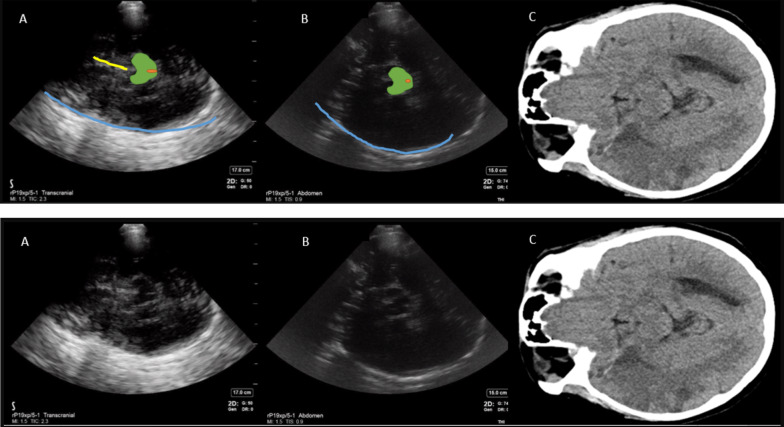
Materials and methods: After obtaining IRB approval, a blinded investigator performed cranial ultrasound (Fujifilm, Sonosite® Xporte, transcranial and abdominal presets) through temporal windows on 11 patients with intracerebral pathology within 72 h of last CT/MRI (computed tomography scan/magnetic resonance imaging) brain after being admitted to a neurocritical care unit in Aug 2020 and Nov 2020-Mar 2021. Images were then compared to patient's CT/MRI to inform topography. Inferential statistics were reported.
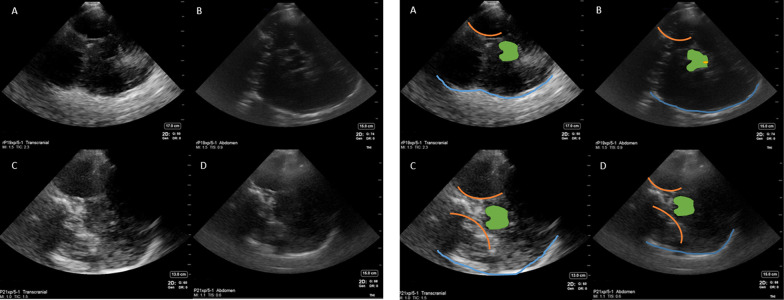
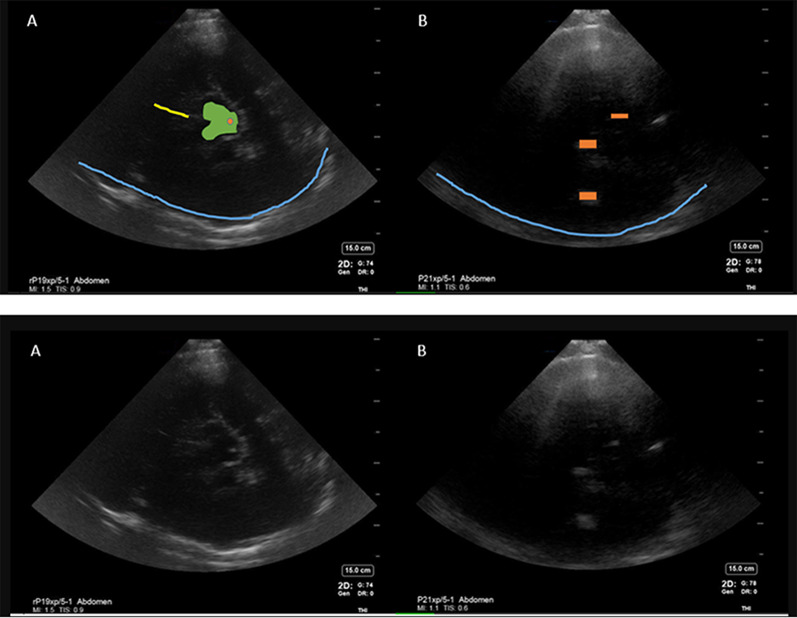
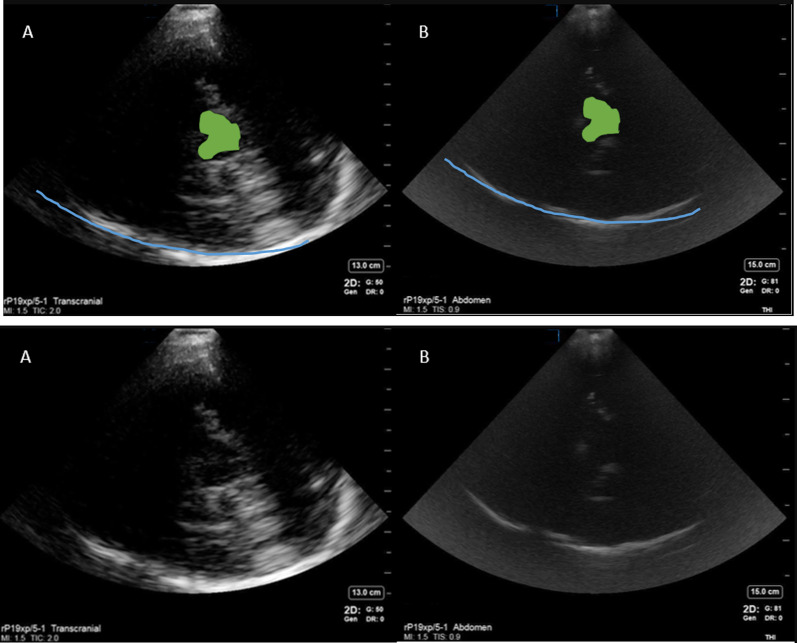
Results: Mean age was 57 (28-77 years) and 6/11 were female. Six patients were diagnosed with ICH, 3 with ischemic stroke, 1 subarachnoid hemorrhage, and 1 brain tumor. The sensitivity and specificity of point of care diagnosis of ICH compared to CT/MRI brain was 100% and 50%, respectively. Mean time between ultrasound scan and CT/MRI was 13.3 h (21 min-39 h). Falx cerebri, choroid calcification and midbrain-related artifacts were the most reproducible hyperechoic signals. Abdominal preset on high gain yielded less artifact than Transcranial Doppler preset for cranial B mode imaging. False positive ICH diagnosis was attributed to intracerebral tumor and midbrain-related artifact.
Conclusions: Our exploratory analysis yielded preliminary data on use of point of care cranial ultrasound for ICH diagnosis to inform imaging techniques, cranial topography on B mode and sample size estimation for future studies to evaluate sensitivity and specificity of cranial POCUS in adult patients. This pilot study is limited by small sample size and over representation of ICH in the study. Cranial POCUS is feasible using POCUS machines and may have potential as a screening tool if validated in adequately powered studies.
Keywords: Brain hemorrhage; Doppler transcranial; Echography; Sonography; Ultrasound imaging.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interest.
Figures
References
-
- Woydt M, Greiner K, Perez J, Becker G, Krone A, Roosen K. Transcranial duplex-sonography in intracranial hemorrhage evaluation of transcranial duplex-sonography in the diagnosis of spontaneous and traumatic intracranial hemorrhage. Zentralblatt Fur Neurochir. 1996;57(3):129–135. - PubMed
LinkOut - more resources
Full Text Sources