

Outcomes of mild-to-moderate postresuscitation shock after non-shockable cardiac arrest and association with temperature management: a post hoc analysis of HYPERION trial data
- PMID: 36251223
- PMCID: PMC9576832
- DOI: 10.1186/s13613-022-01071-z
Outcomes of mild-to-moderate postresuscitation shock after non-shockable cardiac arrest and association with temperature management: a post hoc analysis of HYPERION trial data
Abstract
Background: Outcomes of postresuscitation shock after cardiac arrest can be affected by targeted temperature management (TTM). A post hoc analysis of the "TTM1 trial" suggested higher mortality with hypothermia at 33 °C. We performed a post hoc analysis of HYPERION trial data to assess potential associations linking postresuscitation shock after non-shockable cardiac arrest to hypothermia at 33 °C on favourable functional outcome.
Methods: We divided the patients into groups with vs. without postresuscitation (defined as the need for vasoactive drugs) shock then assessed the proportion of patients with a favourable functional outcome (day-90 Cerebral Performance Category [CPC] 1 or 2) after hypothermia (33 °C) vs. controlled normothermia (37 °C) in each group. Patients with norepinephrine or epinephrine > 1 µg/kg/min were not included.
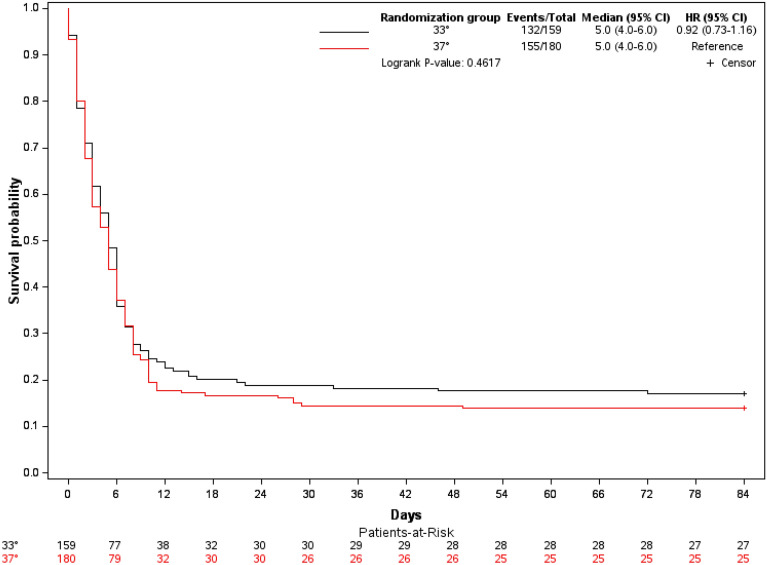
Results: Of the 581 patients included in 25 ICUs in France and who did not withdraw consent, 339 had a postresuscitation shock and 242 did not. In the postresuscitation-shock group, 159 received hypothermia, including 14 with a day-90 CPC of 1-2, and 180 normothermia, including 10 with a day-90 CPC of 1-2 (8.81% vs. 5.56%, respectively; P = 0.24). After adjustment, the proportion of patients with CPC 1-2 also did not differ significantly between the hypothermia and normothermia groups (adjusted hazards ratio, 1.99; 95% confidence interval, 0.72-5.50; P = 0.18). Day-90 mortality was comparable in these two groups (83% vs. 86%, respectively; P = 0.43).
Conclusions: After non-shockable cardiac arrest, mild-to-moderate postresuscitation shock at intensive-care-unit admission did not seem associated with day-90 functional outcome or survival. Therapeutic hypothermia at 33 °C was not associated with worse outcomes compared to controlled normothermia in patients with postresuscitation shock. Trial registration ClinicalTrials.gov, NCT01994772.
Keywords: Cardiac arrest; In-hospital; Postresuscitation shock; Targeted temperature management; Therapeutic hypothermia.
© 2022. The Author(s).
Conflict of interest statement
JB Lascarrou has received reimbursement for travel expenses from Zoll (Voisin Le Bretonneux, France) and BD (Le Pont de Claix, France). JP Frat has received personal fees for lectures, travel expense coverage to attend scientific meetings from Fisher and Paykel Healthcare, and a grant for a randomized controlled trial; personal fees as a member of a scientific board, and travel expense coverage to attend scientific meetings from SOS Oxygène. None of the other authors has any conflict of interest to declare.
Figures
References
-
- Huang C-H, Tsai M-S, Ong HN, Chen W, Wang C-H, Chang W-T, et al. Association of hemodynamic variables with in-hospital mortality and favorable neurological outcomes in post-cardiac arrest care with targeted temperature management. Resuscitation. 2017;120:146–152. doi: 10.1016/j.resuscitation.2017.07.009. - DOI - PubMed
-
- Hästbacka J, Kirkegaard H, Søreide E, Taccone FS, Rasmussen BS, Storm C, et al. Severe or critical hypotension during post cardiac arrest care is associated with factors available on admission—a post hoc analysis of the TTH48 trial. J Crit Care. 2021;61:186–190. doi: 10.1016/j.jcrc.2020.10.026. - DOI - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
