

Postexposure Prophylaxis and Treatment of Bacillus anthracis Infections: A Systematic Review and Meta-analyses of Animal Models, 1947-2019
- PMID: 36251546
- PMCID: PMC9649436
- DOI: 10.1093/cid/ciac591
Postexposure Prophylaxis and Treatment of Bacillus anthracis Infections: A Systematic Review and Meta-analyses of Animal Models, 1947-2019
Abstract
Background: Anthrax is endemic to many countries, including the United States. The causative agent, Bacillus anthracis, poses a global bioterrorism threat. Without effective antimicrobial postexposure prophylaxis (PEPAbx) and treatment, the mortality of systemic anthrax is high. To inform clinical guidelines for PEPAbx and treatment of B. anthracis infections in humans, we systematically evaluated animal anthrax treatment model studies.
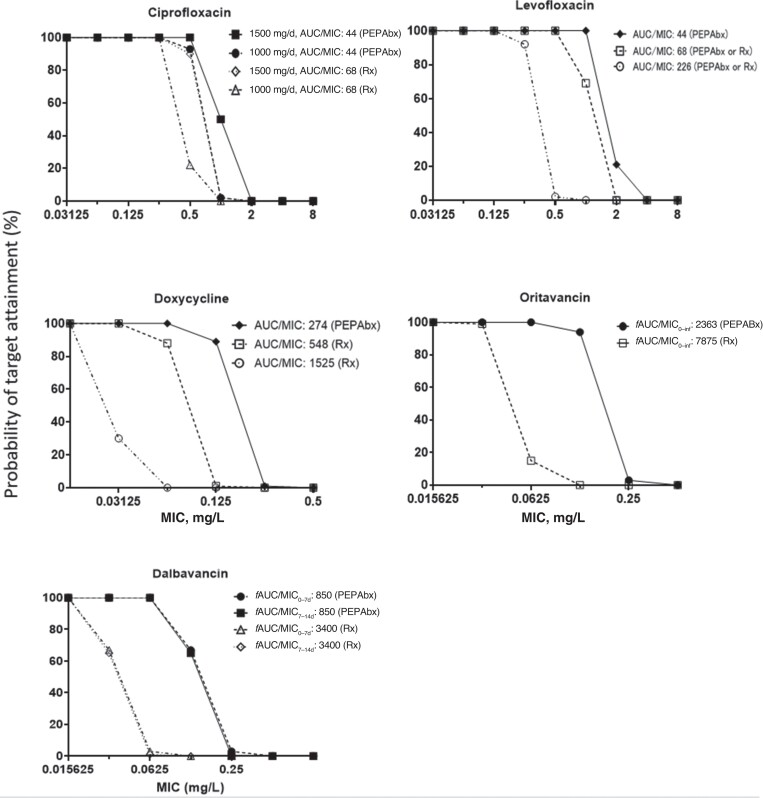
Methods: We searched for survival outcome data in 9 scientific search engines for articles describing antimicrobial PEPAbx or treatment of anthrax in animals in any language through February 2019. We performed meta-analyses of efficacy of antimicrobial PEPAbx and treatment for each drug or drug combination using random-effects models. Pharmacokinetic/pharmacodynamic relationships were developed for 5 antimicrobials with available pharmacokinetic data. Monte Carlo simulations were used to predict unbound drug exposures in humans.
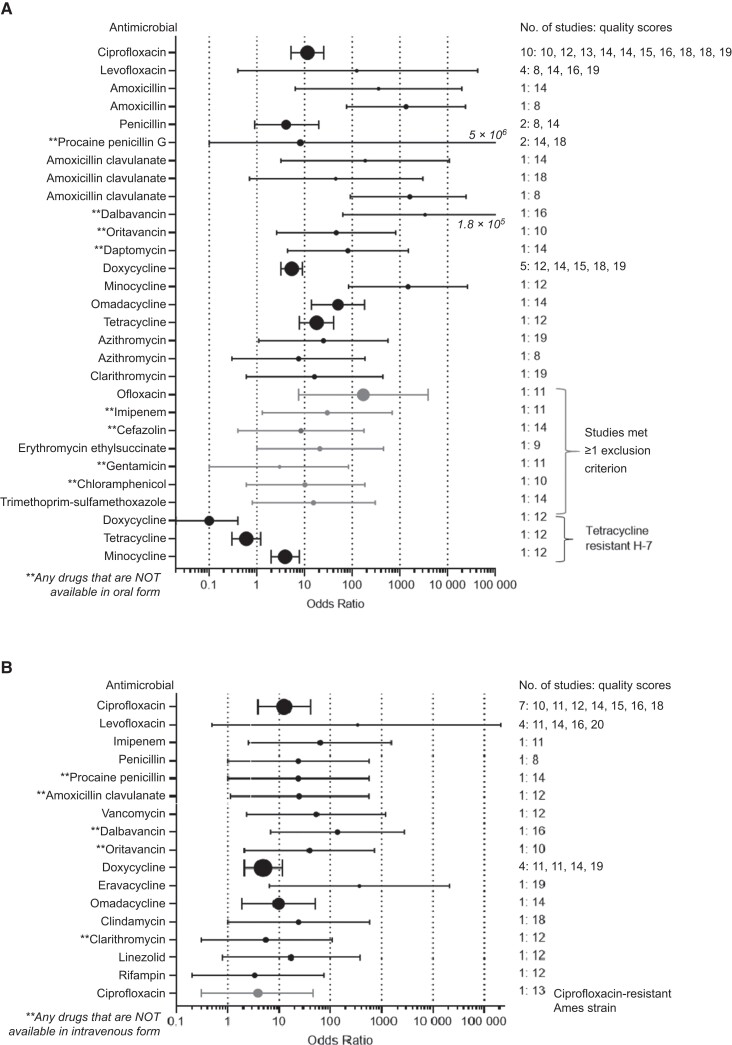
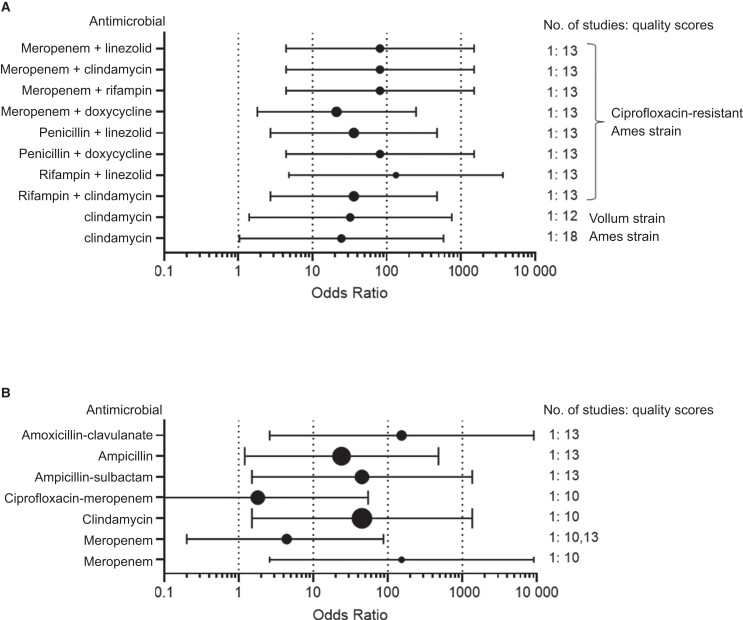
Results: We synthesized data from 34 peer-reviewed studies with 3262 animals. For PEPAbx and treatment of infection by susceptible B. anthracis, effective monotherapy can be accomplished with fluoroquinolones, tetracyclines, β-lactams (including penicillin, amoxicillin-clavulanate, and imipenem-cilastatin), and lipopeptides or glycopeptides. For naturally occurring strains, unbound drug exposures in humans were predicted to adequately cover the minimal inhibitory concentrations (MICs; those required to inhibit the growth of 50% or 90% of organisms [MIC50 or MIC90]) for ciprofloxacin, levofloxacin, and doxycycline for both the PEPAbx and treatment targets. Dalbavancin covered its MIC50 for PEPAbx.
Conclusions: These animal studies show many reviewed antimicrobials are good choices for PEPAbx or treatment of susceptible B. anthracis strains, and some are also promising options for combating resistant strains. Monte Carlo simulations suggest that oral ciprofloxacin, levofloxacin, and doxycycline are particularly robust choices for PEPAbx or treatment.
Keywords: anthrax; antimicrobial; drug-resistant; postexposure prophylaxis; treatment.
Published by Oxford University Press on behalf of Infectious Diseases Society of America 2022.
Figures
References
-
- Carlson CJ, Kracalik IT, Ross N, et al. The global distribution of Bacillus anthracis and associated anthrax risk to humans, livestock and wildlife. Nat Microbiol 2019; 4:1337–43. - PubMed
-
- Athamna A, Athamna M, Abu-Rashed N, Medlej B, Bast DJ, Rubinstein E. Selection of Bacillus anthracis isolates resistant to antibiotics. J Antimicrob Chemother 2004; 54:424–8. - PubMed
-
- Meselson M, Guillemin J, Hugh-Jones M, et al. The Sverdlovsk anthrax outbreak of 1979. Science 1994; 266:1202–8. - PubMed
-
- Holty JE, Bravata DM, Liu H, Olshen RA, McDonald KM, Owens DK. Systematic review: a century of inhalational anthrax cases from 1900 to 2005. Ann Intern Med 2006; 144:270–80. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
