

Is There a Wound Recontamination by Eluates with High Bacterial Load in Negative-Pressure Wound Therapy with Instillation and Dwell Time?
- PMID: 36251856
- PMCID: PMC9788932
- DOI: 10.1097/PRS.0000000000009770
Is There a Wound Recontamination by Eluates with High Bacterial Load in Negative-Pressure Wound Therapy with Instillation and Dwell Time?
Abstract
Background: This study investigated bacterial colonization of the foam eluate after negative-pressure wound therapy (NPWT) with instillation and dwell time (NPWTi-d) to obtain an indication of possible recontamination of the wound during NPWTi-d. To detect bacterial colonization and the extent of planktonic and nonplanktonic bioburden as comprehensively as possible, routine culture and molecular biology methods were used.
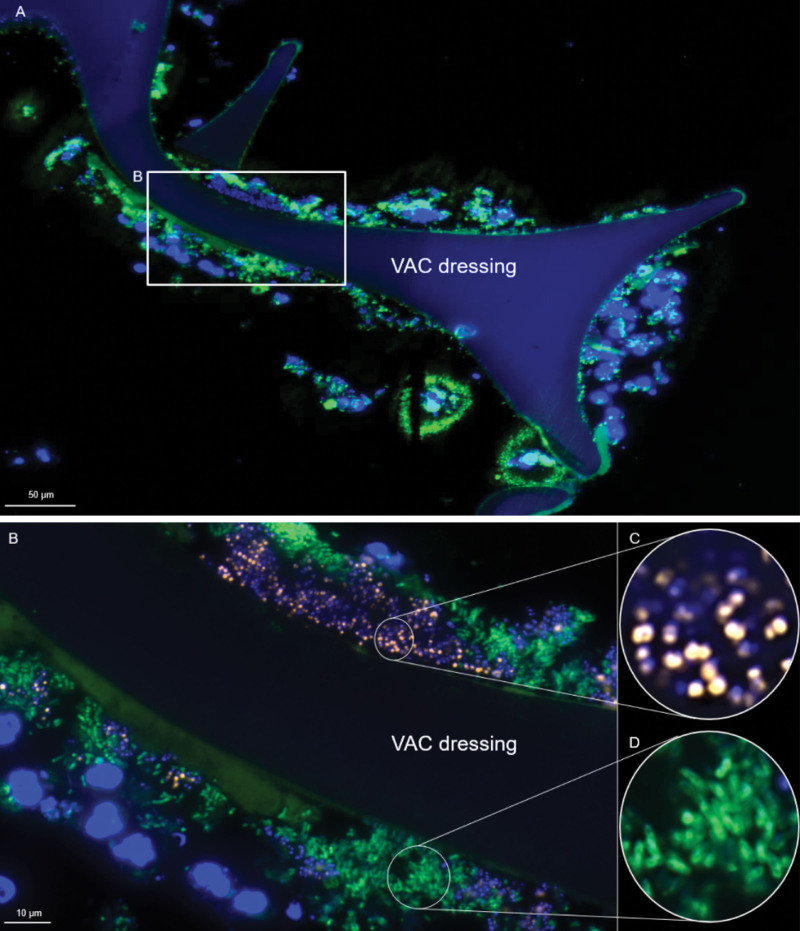
Methods: Before (time point 1) and after (median 3.0 days; time point 2) NPWT ( n = 15) and NPWTi-d with antiseptic installation ( n = 15), wound bed [22 acute, eight chronic wounds; median age, 51 years (range, 24 to 91); 26 men], foam, and eluate were examined by routine culture methods and fluorescence in situ hybridization (FISH), polymerase chain reaction, and FISH sequencing (FISHseq).
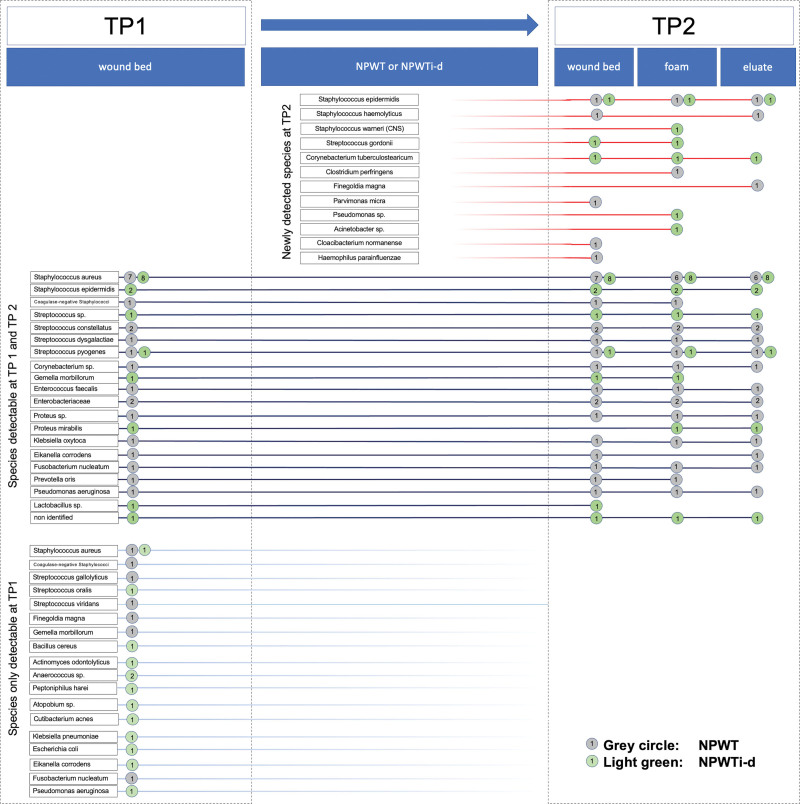
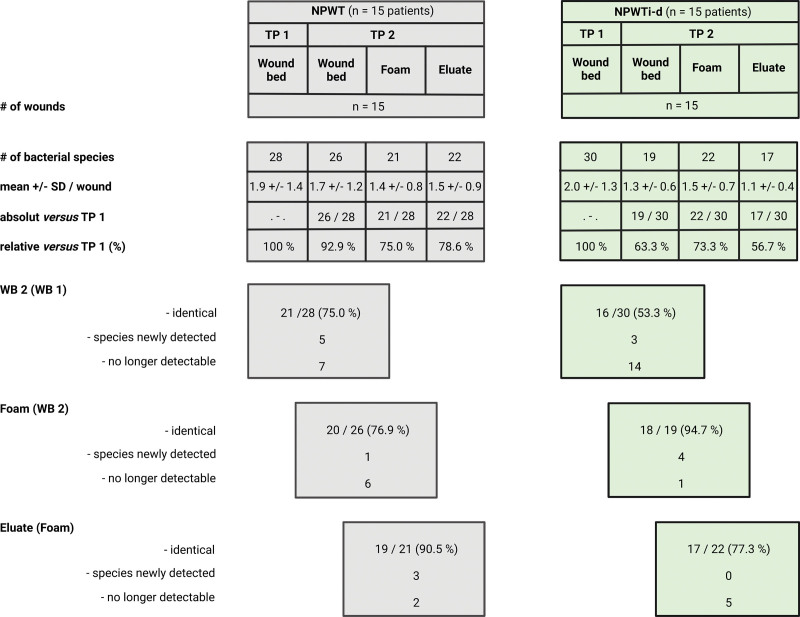
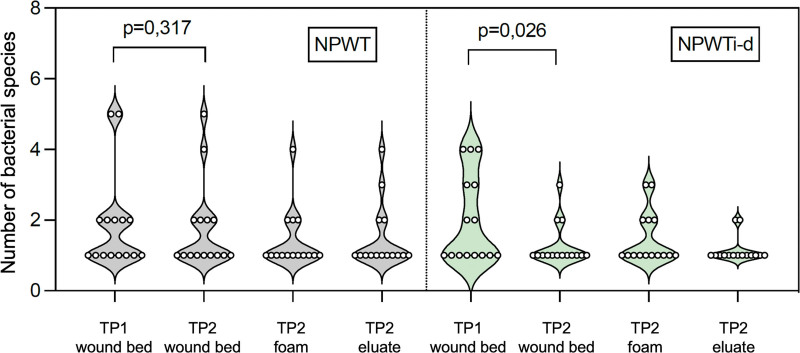
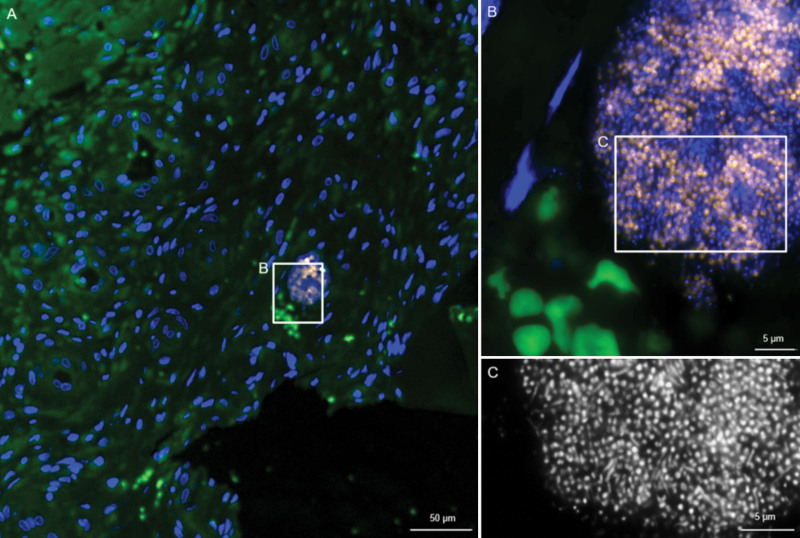
Results: At time point 2, 94.9% (37 of 39) of the pathogens identifiable in the eluate were also detected in the wound bed. Foam and eluate were always bacterially contaminated. NPWTi-d resulted in a significant reduction in the number of pathogen species compared with NPWT (NPWTi-d, time point 1 versus time point 2: P = 0.026; NPWT, time point 1 versus time point 2: not significant). Routine culture of wound bed samples at time point 2 identified only 28 of 52 (53.8%) of the pathogens, whereas examination of wound bed, foam, and eluate and additional FISHseq use detected 50 of 52 (96.2%) of the bacterial species. FISHseq identified biofilm in one and microcolonies in 10 wounds (time point 2).
Conclusions: The bacterial load of the foam is flushed back into the wound during NPWTi-d. FISHseq should be used in addition to the routine culture method when pathogen identification and detection of nonplanktonic bacterial growth is particularly important for the patient's therapy.
Clinical question/level of evidence: Therapeutic, V.
Copyright © 2022 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the American Society of Plastic Surgeons. All rights reserved.
Figures
References
-
- Téot L, Guillot-Masanovic M, Miquel P, et al. . Clinical impact of negative-pressure wound therapy: a 1,126-patient observational prospective study. Wound Repair Regen. 2014;22:341–350. - PubMed
-
- Apelqvist J, Willy C, Fagerdahl AM, et al. . EWMA document: negative pressure wound therapy. J Wound Care. 2017;26(Suppl 3):S1–S154. - PubMed
-
- Moch D, Fleischmann W, Westhauser A. [Instillation vacuum sealing: report of initial experiences.] Langenbecks Arch Chir Suppl Kongressbd. 1998;115:1197–1199. - PubMed
-
- Timmers MS, Graafland N, Bernards AT, Nelissen RG, van Dissel JT, Jukema GN. Negative pressure wound treatment with polyvinyl alcohol foam and polyhexanide antiseptic solution instillation in posttraumatic osteomyelitis. Wound Repair Regen. 2009;17:278–286. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
