

Blood Pressure and Cardiorenal Outcomes With Finerenone in Chronic Kidney Disease in Type 2 Diabetes
- PMID: 36252131
- PMCID: PMC9640256
- DOI: 10.1161/HYPERTENSIONAHA.122.19744
Blood Pressure and Cardiorenal Outcomes With Finerenone in Chronic Kidney Disease in Type 2 Diabetes
Abstract
Background: Chronic kidney disease is frequently associated with hypertension and poorly controlled blood pressure can lead to chronic kidney disease progression. Finerenone, a nonsteroidal mineralocorticoid receptor antagonist, significantly improves cardiorenal outcomes in patients with chronic kidney disease and type 2 diabetes. This analysis explored the relationship between office systolic blood pressure (SBP) and cardiorenal outcomes with finerenone in FIDELIO-DKD trial (Finerenone in Reducing Kidney Failure and Disease Progression in Diabetic Kidney Disease).
Methods: Patients with type 2 diabetes, urine albumin-to-creatinine ratio 30 to 5000 mg/g, and estimated glomerular filtration rate of 25 to <75 mL/min per 1.73 m2 receiving optimized renin-angiotensin system blockade, were randomized to finerenone or placebo. For this analysis, patients (N=5669) were grouped by baseline office SBP quartiles.
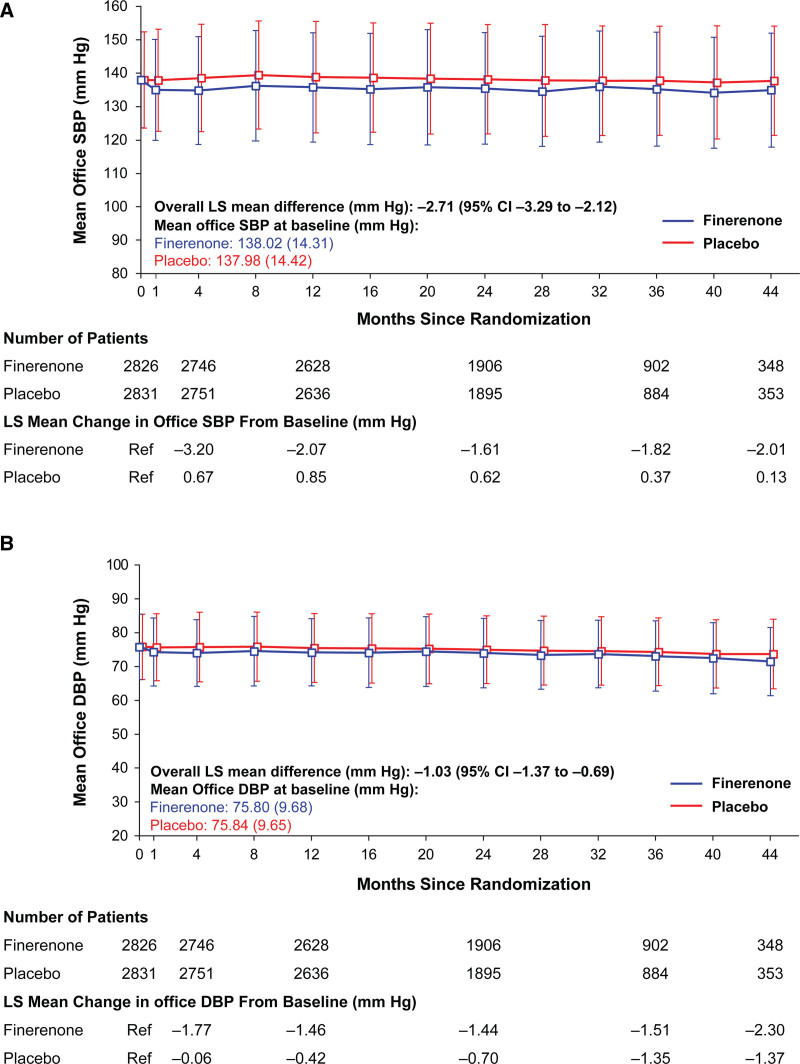
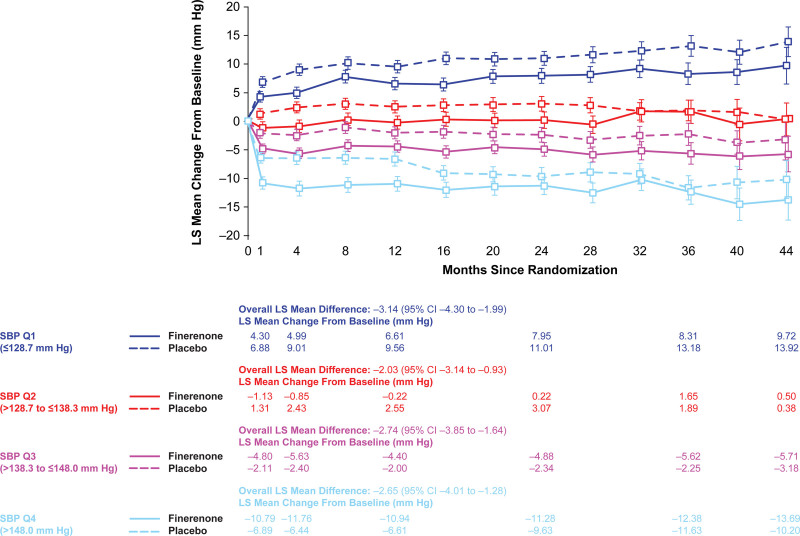
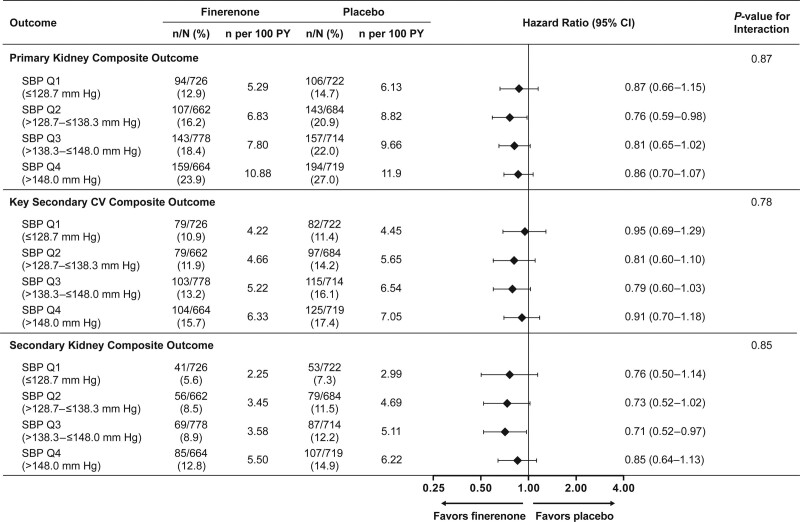
Results: Finerenone reduced office SBP across the baseline office SBP quartiles, including patients with baseline office SBP of >148 mm Hg. Overall, patients with lower baseline office SBP quartile and greater declines from baseline in SBP were associated with better cardiorenal outcomes. The risk of primary kidney and key secondary cardiovascular composite outcomes was consistently reduced with finerenone versus placebo irrespective of baseline office SBP quartiles (P for interaction 0.87 and 0.78, respectively). A time-varying analysis revealed that 13.8% and 12.6% of the treatment effect with finerenone was attributed to the change in office SBP for the primary kidney composite outcome and the key secondary cardiovascular outcome, respectively.
Conclusions: In FIDELIO-DKD, cardiorenal outcomes improved with finerenone irrespective of baseline office SBP. Reductions in office SBP accounted for a small proportion of the treatment effect on cardiorenal outcomes.
Registration: URL: https://www.
Clinicaltrials: gov; Unique identifier: NCT02540993.
Keywords: blood pressure; chronic kidney diseases; finerenone; mineralocorticoid receptor antagonist; systolic blood pressure; type 2 diabetes.
Figures
References
-
- Ku E, Lee BJ, Wei J, Weir MR. Hypertension in CKD: core curriculum 2019. Am J Kidney Dis. 2019;74:120–131. doi: 10.1053/j.ajkd.2018.12.044 - PubMed
-
- Levey AS, Astor BC, Stevens LA, Coresh J. Chronic kidney disease, diabetes, and hypertension: what’s in a name?. Kidney Int. 2010;78:19–22. doi: 10.1038/ki.2010.115 - PubMed
-
- Sarafidis PA, Ruilope LM. Aggressive blood pressure reduction and renin-angiotensin system blockade in chronic kidney disease: time for re-evaluation?. Kidney Int. 2014;85:536–546. doi: 10.1038/ki.2013.355 - PubMed
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Blood Pressure Work Group. KDIGO 2021 clinical practice guideline for the management of blood pressure in chronic kidney disease. Kidney Int. 2021;99:S1–S87. doi: 10.1016/j.kint.2020.11.003 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
