

Lipoprotein(a) levels in a global population with established atherosclerotic cardiovascular disease
- PMID: 36252994
- PMCID: PMC9577925
- DOI: 10.1136/openhrt-2022-002060
Lipoprotein(a) levels in a global population with established atherosclerotic cardiovascular disease
Erratum in
-
Correction: Lipoprotein(a) levels in a global population with established atherosclerotic cardiovascular disease.Open Heart. 2022 Nov;9(2):e002060corr1. doi: 10.1136/openhrt-2022-002060corr1. Open Heart. 2022. PMID: 36384881 Free PMC article. No abstract available.
Abstract
Objective: Lipoprotein(a) (Lp(a)) is an important genetically determined risk factor for atherosclerotic vascular disease (ASCVD). With the development of Lp(a)-lowering therapies, this study sought to characterise patterns of Lp(a) levels in a global ASCVD population and identify racial, ethnic, regional and gender differences.
Methods: A multicentre cross-sectional epidemiological study to estimate the prevalence of elevated Lp(a) in patients with a history of myocardial infarction, ischaemic stroke or peripheral artery disease conducted at 949 sites in 48 countries in North America, Europe, Asia, South America, South Africa and Australia between April 2019 and July 2021. Low-density lipoprotein cholesterol (LDL-C) and Lp(a) levels were measured either as mass (mg/dL) or molar concentration (nmol/L).
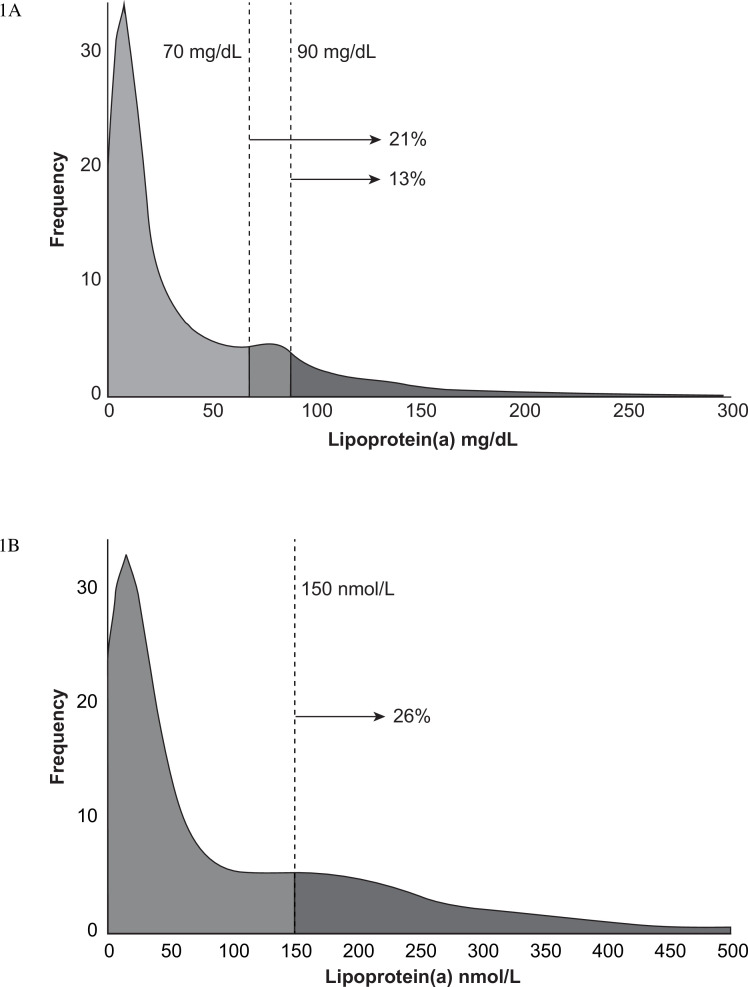
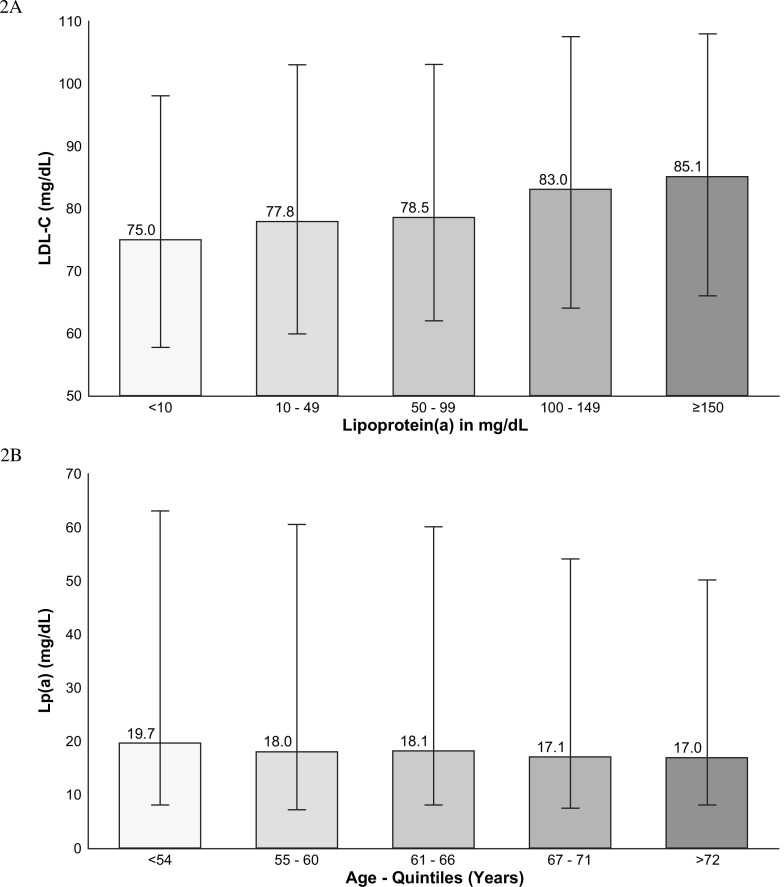
Results: Of 48 135 enrolled patients, 13.9% had prior measurements of Lp(a). Mean age was 62.6 (SD 10.1) years and 25.9% were female. Median Lp(a) was 18.0 mg/dL (IQR 7.9-57.1) or 42.0 nmol/L (IQR 15.0-155.4). Median LDL-C was 77 mg/dL (IQR 58.4-101.0). Lp(a) in women was higher, 22.8 (IQR 9.0-73.0) mg/dL, than in men, 17.0 (IQR 7.1-52.2) mg/dL, p<0.001. Black patients had Lp(a) levels approximately threefold higher than white, Hispanic or Asian patients. Younger patients also had higher levels. 27.9% of patients had Lp(a) levels >50 mg/dL, 20.7% had levels >70 mg/dL, 12.9% were >90 mg/dL and 26.0% of patients exceeded 150 nmol/L.
Conclusions: Globally, Lp(a) is measured in a small minority of patients with ASCVD and is highest in black, younger and female patients. More than 25% of patients had levels exceeding the established threshold for increased cardiovascular risk, approximately 50 mg/dL or 125 nmol/L.
Keywords: atherosclerosis; global burden of disease; hyperlipidemias.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: SEN reports receiving clinical trial support from Novartis and Silence Theapeutics; BN reports consultancies or talks sponsored by AstraZeneca, Sanofi, Regeneron, Akcea, Amgen, Kowa, Denka, Amarin, Novartis, Novo Nordisk, Esperion and Silence Therapeutics.
Figures
References
-
- Grundy SM, Stone NJ, Bailey AL, et al. . 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2019;73:e285–350. 10.1016/j.jacc.2018.11.003 - DOI - PubMed
-
- The task force for the management of dyslipidaemias of the European Society of cardiology (ESC) and European atherosclerosis Society (EAS). 2019 ESC/EAS guidelines for themanagement of dyslipidaemias: lipid modification to reduce cardiovascular risk. European Heart Journal 2020;41:188. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous