

Preterm birth and prescriptions for cardiovascular, antiseizure, antibiotics and antiasthmatic medication in children up to 10 years of age: a population-based data linkage cohort study across six European regions
- PMID: 36253045
- PMCID: PMC9577906
- DOI: 10.1136/bmjopen-2022-061746
Preterm birth and prescriptions for cardiovascular, antiseizure, antibiotics and antiasthmatic medication in children up to 10 years of age: a population-based data linkage cohort study across six European regions
Abstract
Objectives: Preterm children are exposed to many medications in neonatal intensive care units, but little is known about the effect of prematurity on medication use throughout infancy and childhood. We examined prescriptions of cardiovascular medication (CVM), antiseizure medication (ASM), antiasthmatic medication and antibiotics issued/dispensed in the first 10 years of life for very and moderately preterm children compared with term.
Design: Population-based data linkage cohort study linking information from birth records to prescription records.
Setting: Six registries from five countries in the EUROlinkCAT study.
Participants: The study population included 1 722 912 children, of whom 10 820 (0.6%) were very preterm (<32 weeks gestational age (GA)), 92 814 (5.4%) were moderately preterm (32-36 weeks GA), 1 606 643 (93.3%) were born at term (≥37 weeks GA) and 0.7% had missing GA. Children with major or minor congenital anomalies were excluded (including patent ductus arteriosus).
Main outcome measures: Relative risk (RR) of receiving a prescription for CVM, ASM, antiasthmatic and antibiotics.
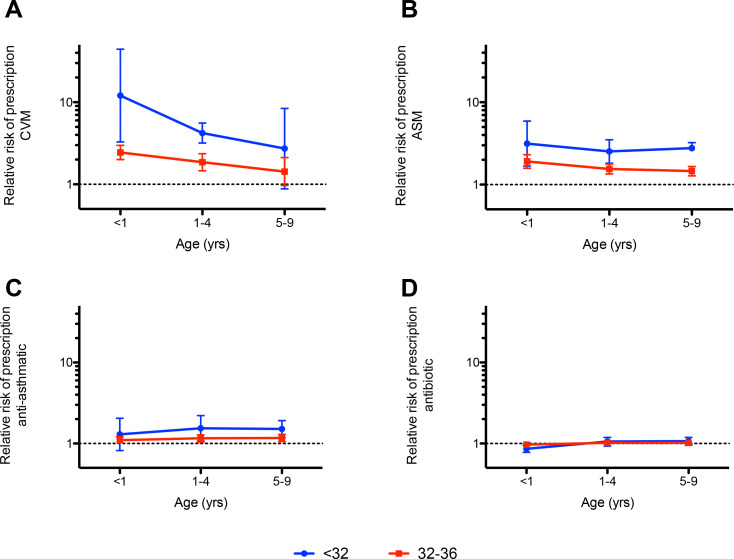
Results: Very preterm children had a higher RR of receiving a prescription for CVM and ASM than preterm children. For all preterm children, the RR of having a CVM prescription was 3.58 (95% CI 2.06 to 6.23); 2.06 (95% CI 1.73 to 2.41) for ASM; 1.13 (95% CI 0.99 to 1.29) for antiasthmatics and 0.96 (95% CI 0.93 to 0.99) for antibiotics in the first year of life. Increased prescription of CVM, ASM and antiasthmatics persisted for all 10 years of follow-up. Although the RR was highest for CVM and ASM, in absolute numbers more children received prescriptions for antibiotics (42.34%, 95% CI 38.81% to 45.91%) and antiasthmatics (28.40%, 95% CI 16.07% to 42.649%) than for CVM (0.18%, 95% CI 0.12% to 0.25%) and ASM (0.16%, 95% CI 0.13% to 0.20%) in the first year of life.
Conclusion: Preterm children had a higher risk of being prescribed/dispensed CVM, ASM and antiasthmatics up to age 10. This study highlights a need for further research into morbidity beyond age 10.
Keywords: Congenital heart disease; NEONATOLOGY; Public health.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources