

Incorporation of Serial 12-Lead Electrocardiogram With Machine Learning to Augment the Out-of-Hospital Diagnosis of Non-ST Elevation Acute Coronary Syndrome
- PMID: 36253296
- PMCID: PMC9780162
- DOI: 10.1016/j.annemergmed.2022.08.005
Incorporation of Serial 12-Lead Electrocardiogram With Machine Learning to Augment the Out-of-Hospital Diagnosis of Non-ST Elevation Acute Coronary Syndrome
Abstract
Study objective: Ischemic electrocardiogram (ECG) changes are subtle and transient in patients with suspected non-ST-segment elevation (NSTE)-acute coronary syndrome. However, the out-of-hospital ECG is not routinely used during subsequent evaluation at the emergency department. Therefore, we sought to compare the diagnostic performance of out-of-hospital and ED ECG and evaluate the incremental gain of artificial intelligence-augmented ECG analysis.
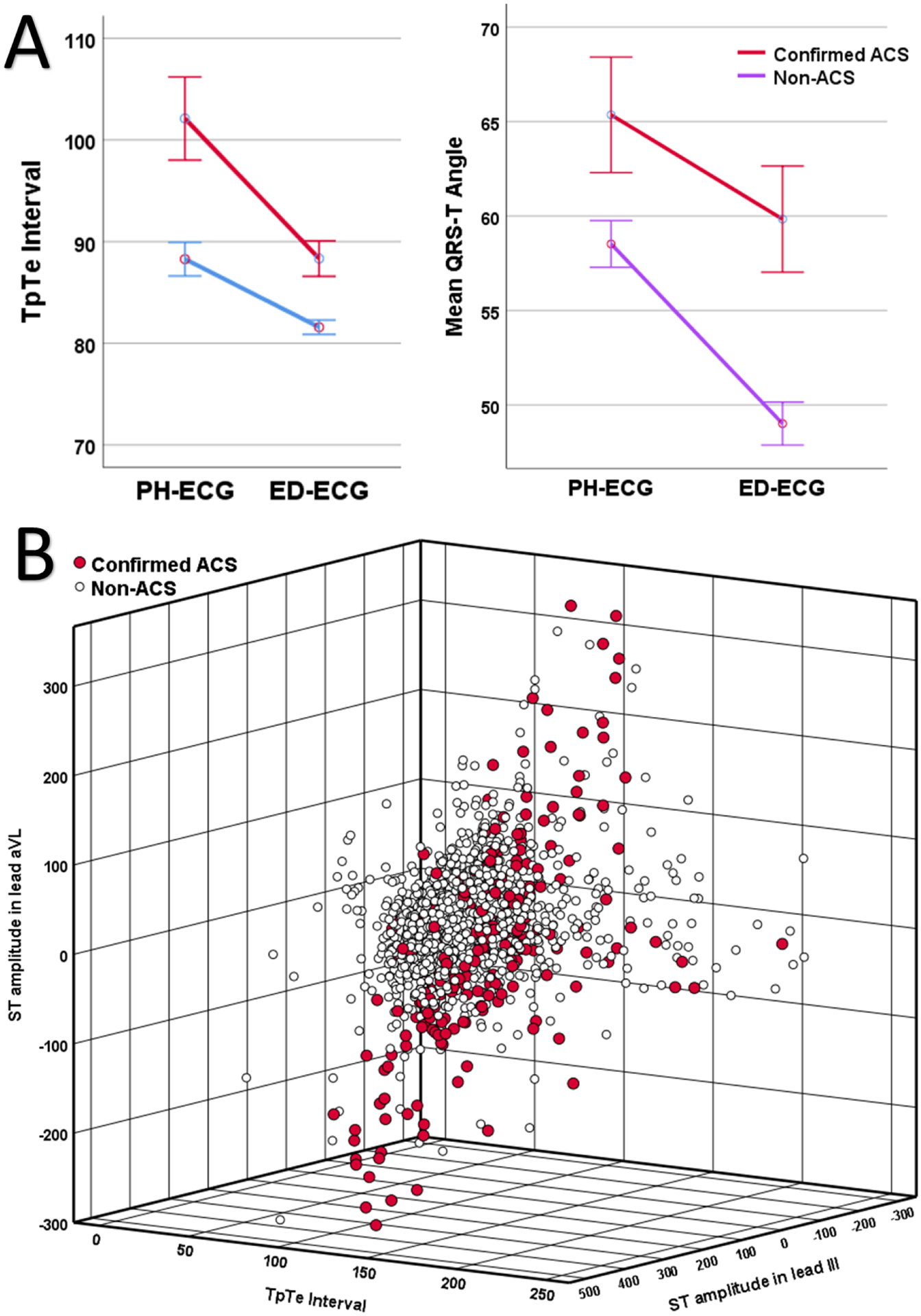
Methods: This prospective observational cohort study recruited patients with out-of-hospital chest pain. We retrieved out-of-hospital-ECG obtained by paramedics in the field and the first ED ECG obtained by nurses during inhospital evaluation. Two independent and blinded reviewers interpreted ECG dyads in mixed order per practice recommendations. Using 179 morphological ECG features, we trained, cross-validated, and tested a random forest classifier to augment non ST-elevation acute coronary syndrome (NSTE-ACS) diagnosis.
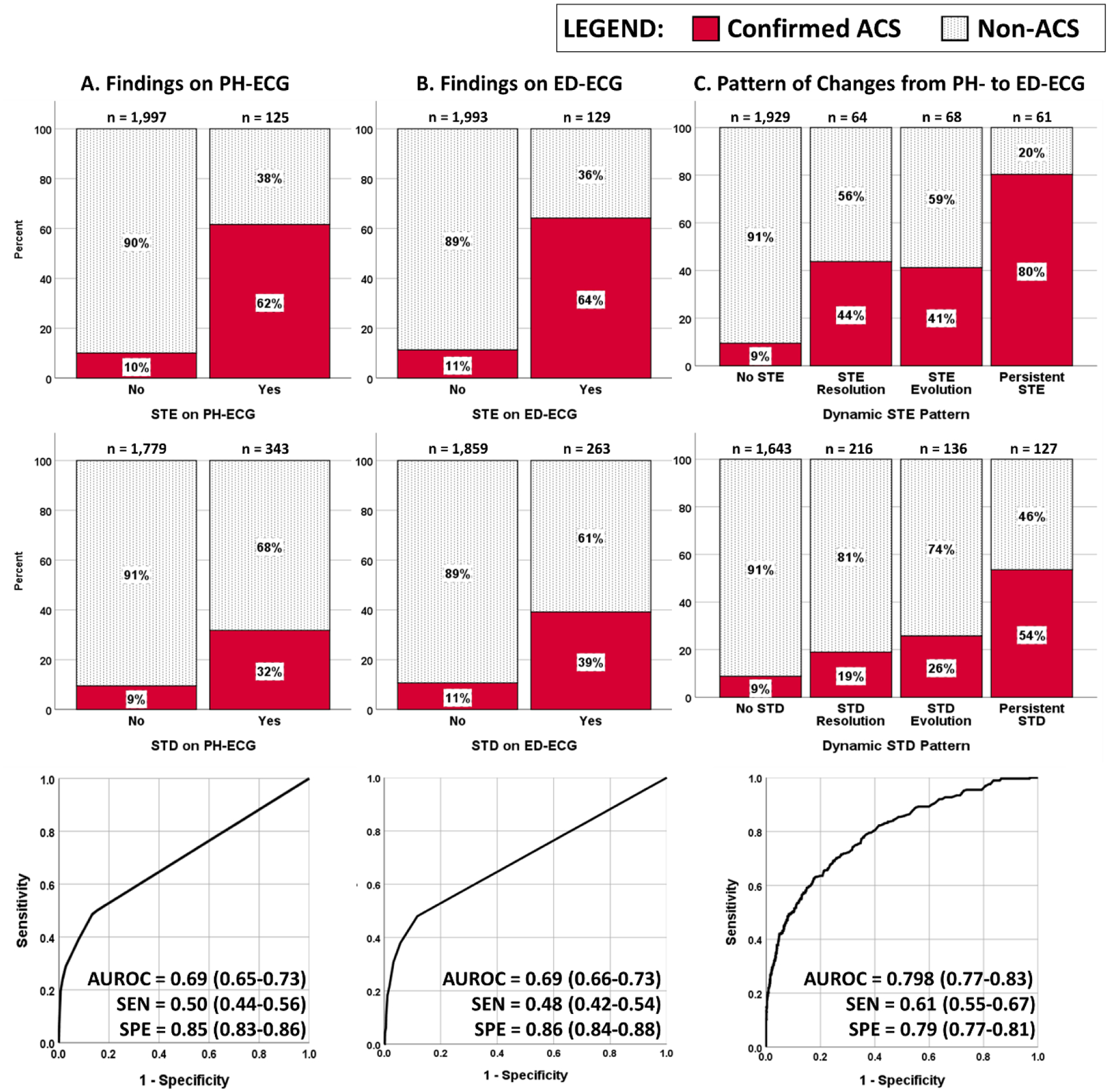
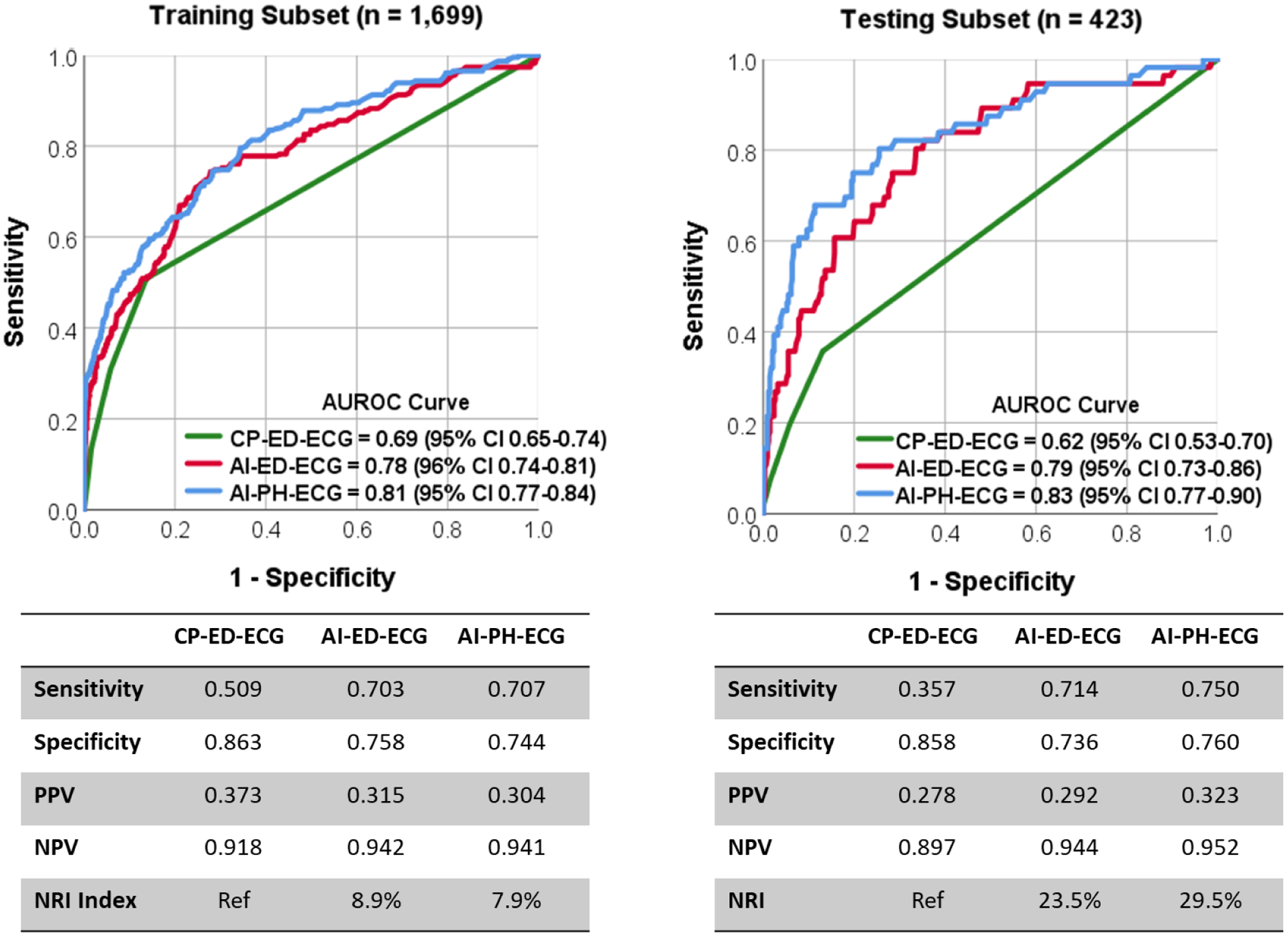
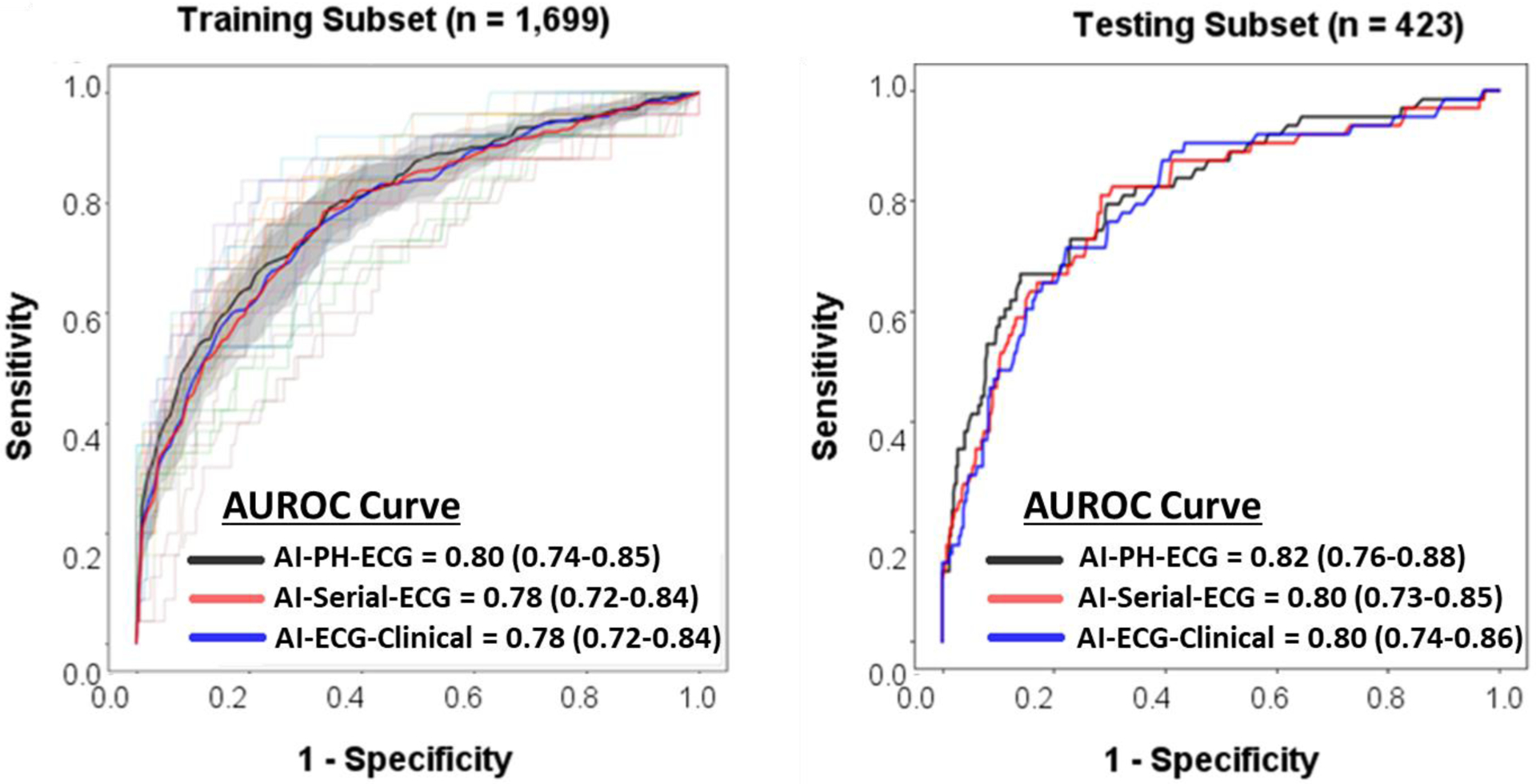
Results: Our sample included 2,122 patients (age 59 [16]; 53% women; 44% Black, 13.5% confirmed acute coronary syndrome). The rate of diagnostic ST elevation and ST depression were 5.9% and 16.2% on out-of-hospital-ECG and 6.1% and 12.4% on ED ECG, with ∼40% of changes seen on out-of-hospital-ECG persisting and ∼60% resolving. Using expert interpretation of out-of-hospital-ECG alone gave poor baseline performance with area under the receiver operating characteristic (AUC), sensitivity, and negative predictive values of 0.69, 0.50, and 0.92. Using expert interpretation of serial ECG changes enhanced this performance (AUC 0.80, sensitivity 0.61, and specificity 0.93). Interestingly, augmenting the out-of-hospital-ECG alone with artificial intelligence algorithms boosted its performance (AUC 0.83, sensitivity 0.75, and specificity 0.95), yielding a net reclassification improvement of 29.5% against expert ECG interpretation.
Conclusion: In this study, 60% of diagnostic ST changes resolved prior to hospital arrival, making the ED ECG suboptimal for the inhospital evaluation of NSTE-ACS. Using serial ECG changes or incorporating artificial intelligence-augmented analyses would allow correctly reclassifying one in 4 patients with suspected NSTE-ACS.
Trial registration: ClinicalTrials.gov NCT04237688.
Copyright © 2022 American College of Emergency Physicians. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Niska R, Bhuiya F, Xu J. National Hospital Ambulatory Medical Care Survey: 2007 emergency department summary. Natl Health Stat Report. 2010(26):1–31. - PubMed
-
- Gulati M, Levy PD, Mukherjee D, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;144(22):e368–e454. - PubMed
-
- O’Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127(4):e362–425. - PubMed
-
- Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119–177. - PubMed
-
- Bradley EH, Herrin J, Wang Y, et al. Strategies for reducing the door-to-balloon time in acute myocardial infarction. N Engl J Med. 2006;355(22):2308–2320. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
