

SARS-COV-2 antibody responses to AZD1222 vaccination in West Africa
- PMID: 36253377
- PMCID: PMC9574797
- DOI: 10.1038/s41467-022-33792-x
SARS-COV-2 antibody responses to AZD1222 vaccination in West Africa
Abstract
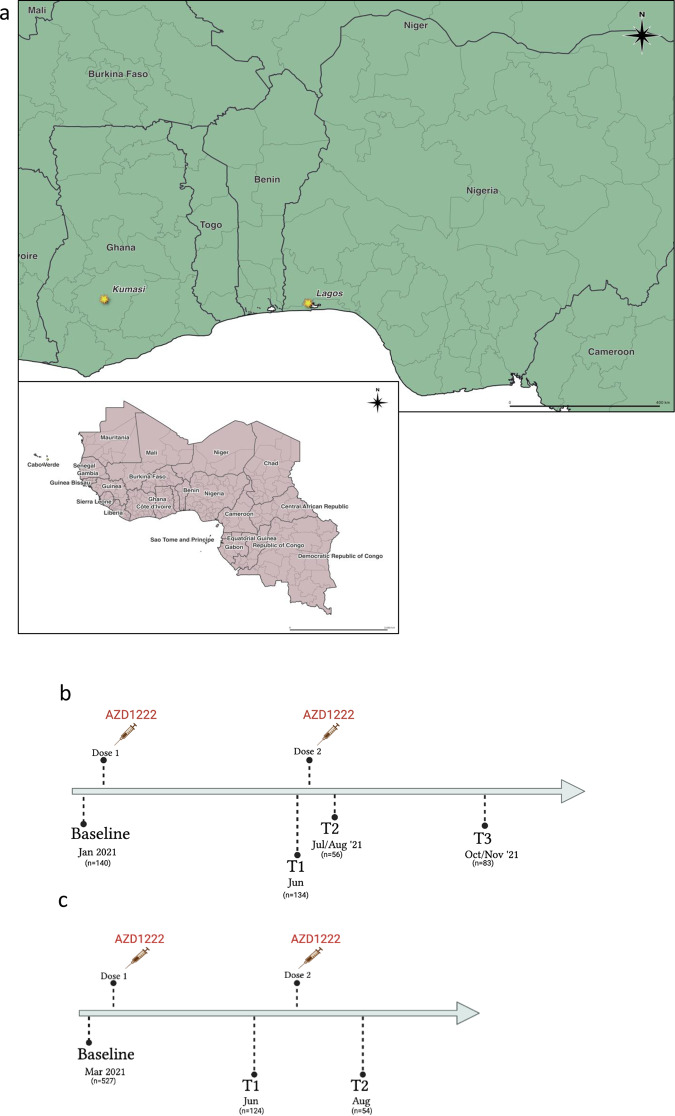
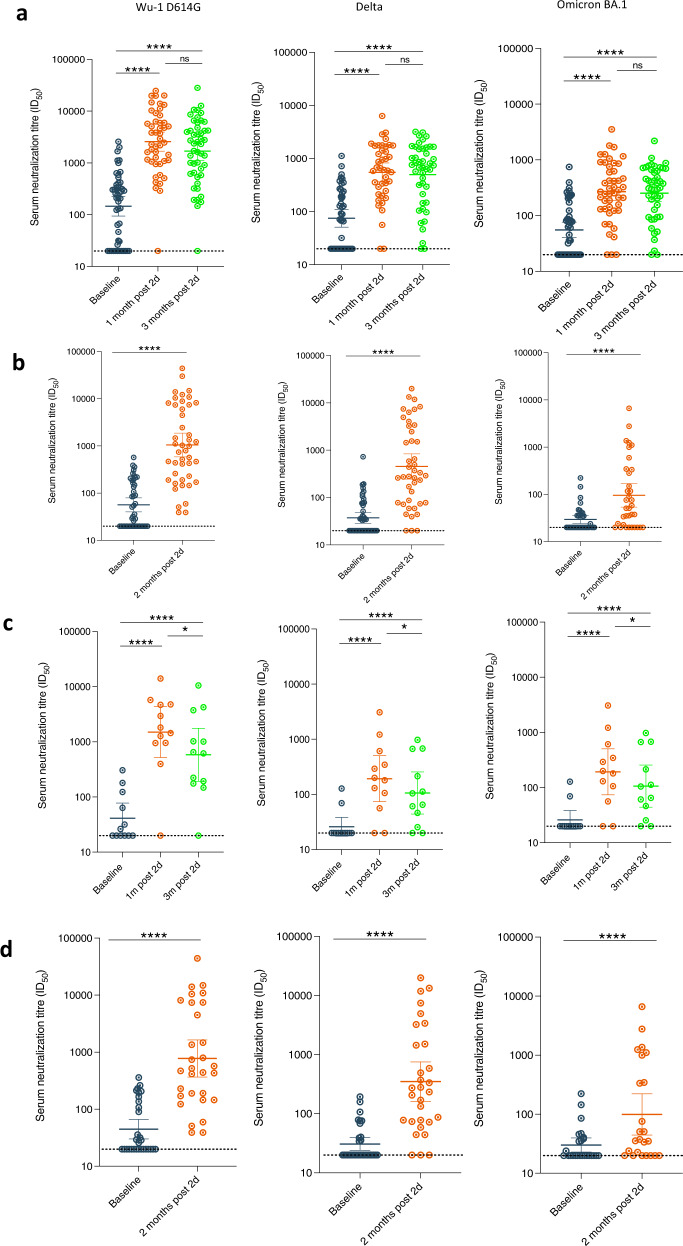
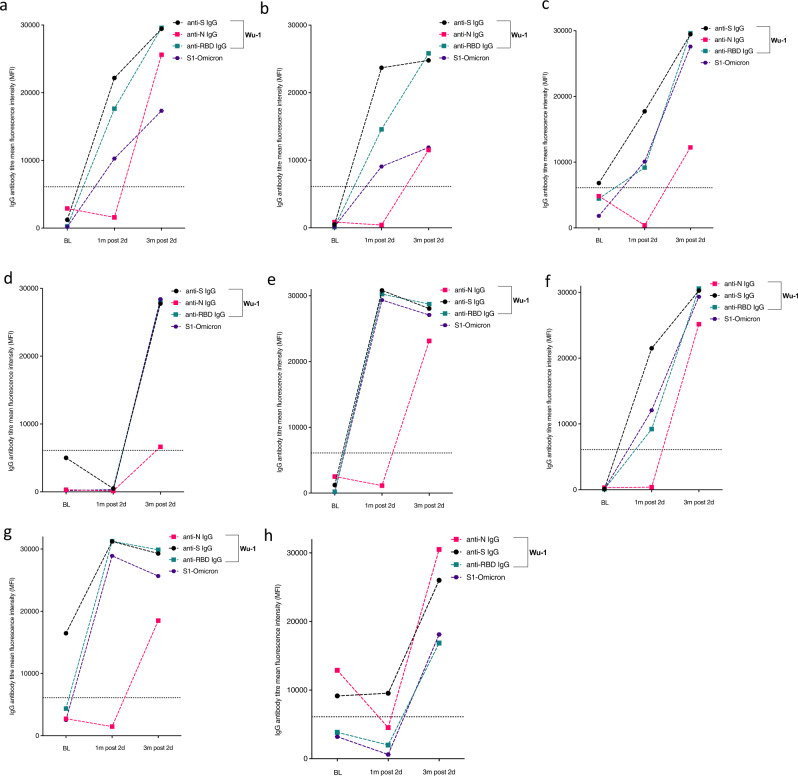
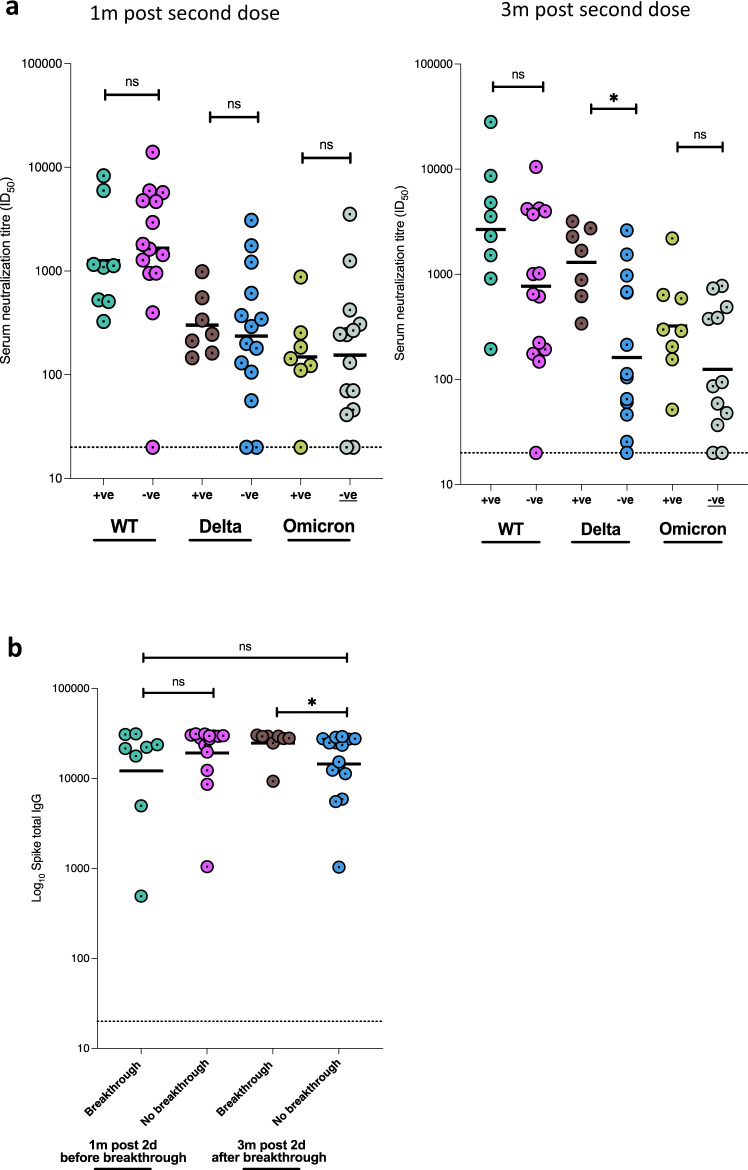
Real-world data on vaccine-elicited neutralising antibody responses for two-dose AZD1222 in African populations are limited. We assessed baseline SARS-CoV-2 seroprevalence and levels of protective neutralizing antibodies prior to vaccination rollout using binding antibodies analysis coupled with pseudotyped virus neutralisation assays in two cohorts from West Africa: Nigerian healthcare workers (n = 140) and a Ghanaian community cohort (n = 527) pre and post vaccination. We found 44 and 28% of pre-vaccination participants showed IgG anti-N positivity, increasing to 59 and 39% respectively with anti-receptor binding domain (RBD) IgG-specific antibodies. Previous IgG anti-N positivity significantly increased post two-dose neutralizing antibody titres in both populations. Serological evidence of breakthrough infection was observed in 8/49 (16%). Neutralising antibodies were observed to wane in both populations, especially in anti-N negative participants with an observed waning rate of 20% highlighting the need for a combination of additional markers to characterise previous infection. We conclude that AZD1222 is immunogenic in two independent West African cohorts with high background seroprevalence and incidence of breakthrough infection in 2021. Waning titres post second dose indicates the need for booster dosing after AZD1222 in the African setting despite hybrid immunity from previous infection.
© 2022. The Author(s).
Conflict of interest statement
R.K.G has received honoraria for educational activities from Janssen, Moderna, and GSK.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
