

Therapeutic advances in COVID-19
- PMID: 36253508
- PMCID: PMC9574806
- DOI: 10.1038/s41581-022-00642-4
Therapeutic advances in COVID-19
Erratum in
-
Author Correction: Therapeutic advances in COVID-19.Nat Rev Nephrol. 2023 Apr;19(4):273. doi: 10.1038/s41581-023-00686-0. Nat Rev Nephrol. 2023. PMID: 36747084 Free PMC article. No abstract available.
Abstract
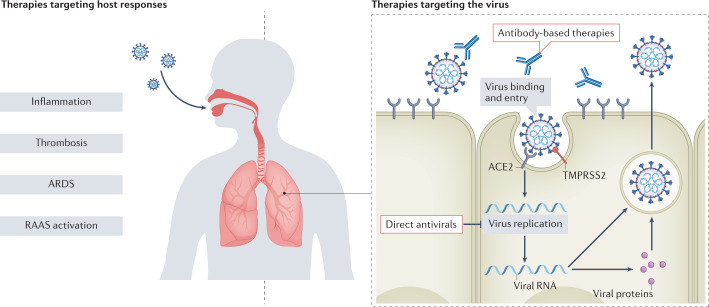
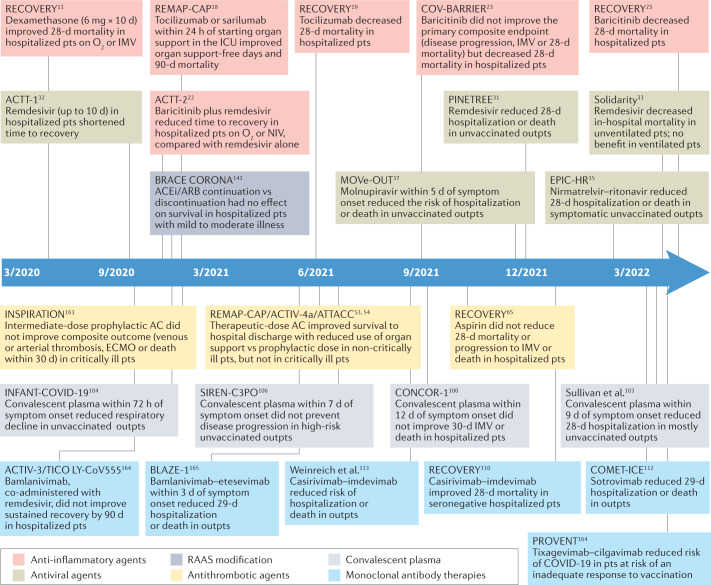
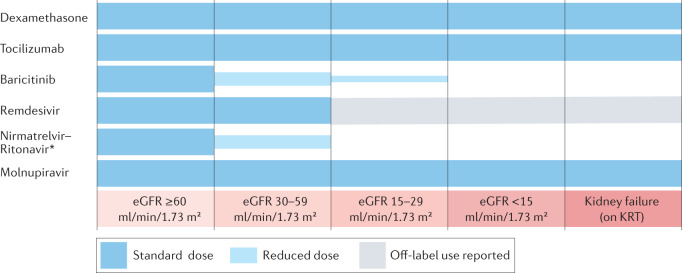
Over 2 years have passed since the start of the COVID-19 pandemic, which has claimed millions of lives. Unlike the early days of the pandemic, when management decisions were based on extrapolations from in vitro data, case reports and case series, clinicians are now equipped with an armamentarium of therapies based on high-quality evidence. These treatments are spread across seven main therapeutic categories: anti-inflammatory agents, antivirals, antithrombotics, therapies for acute hypoxaemic respiratory failure, anti-SARS-CoV-2 (neutralizing) antibody therapies, modulators of the renin-angiotensin-aldosterone system and vitamins. For each of these treatments, the patient population characteristics and clinical settings in which they were studied are important considerations. Although few direct comparisons have been performed, the evidence base and magnitude of benefit for anti-inflammatory and antiviral agents clearly outweigh those of other therapeutic approaches such as vitamins. The emergence of novel variants has further complicated the interpretation of much of the available evidence, particularly for antibody therapies. Importantly, patients with acute and chronic kidney disease were under-represented in many of the COVID-19 clinical trials, and outcomes in this population might differ from those reported in the general population. Here, we examine the clinical evidence for these therapies through a kidney medicine lens.
© 2022. Springer Nature Limited.
Conflict of interest statement
H.A.-S. reports no disclosures relevant to the manuscript; universal disclosures include consultancy (Agios, Dova/Sobi, argenx, Rigel, Novartis, Forma, Moderna) and research funding (Agios, Dova/Sobi, Amgen). P.R.L. is an investigator in the REMAP-CAP ACE2 RAS Domain, which is investigating renin–angiotensin–system-modulating treatments for COVID-19, is supported by a Heart and Stroke Foundation of Canada National New Investigator Award, and has received unrelated consulting honoraria from Novartis, CorEvitas, and Brigham and Women’s Hospital (Boston, MA, USA), as well as unrelated royalties from McGraw-Hill Publishing. L.D.S. is inventor of a patent licensed to SQI Diagnostic and has received unrelated research funding from the Canadian Institutes of Health Research. M.E.S. has received research funding from Gilead Sciences awarded to her institution; additional, unrelated disclosures include research funding from AbbVie, Merck, EMD-Serono, Angion and serving as a scientific advisory board member for Travere and Mallinckrodt. The other authors declare no competing interests.
Figures
Comment in
-
Reply to 'Use of convalescent plasma in the treatment of COVID-19'.Nat Rev Nephrol. 2023 Apr;19(4):272. doi: 10.1038/s41581-023-00691-3. Nat Rev Nephrol. 2023. PMID: 36806371 Free PMC article. No abstract available.
-
Use of convalescent plasma in the treatment of COVID-19.Nat Rev Nephrol. 2023 Apr;19(4):271. doi: 10.1038/s41581-023-00690-4. Nat Rev Nephrol. 2023. PMID: 36806372 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
