

Prevalence, awareness, treatment, and control of type 2 diabetes mellitus among the adult residents of tehran: Tehran Cohort Study
- PMID: 36253738
- PMCID: PMC9578278
- DOI: 10.1186/s12902-022-01161-w
Prevalence, awareness, treatment, and control of type 2 diabetes mellitus among the adult residents of tehran: Tehran Cohort Study
Abstract
Background: The prevalence of type 2 diabetes mellitus has increased in the past decades. We investigated the prevalence of diabetes and its awareness, treatment, and control among adult residents of Tehran.
Methods: We used the recruitment phase data of the Tehran Cohort study, enrolling a random sample of adult residents of Tehran aged ≥35 years. Diabetes was defined as self-report, current use of glucose-lowering medications, and/or fasting plasma glucose (FPG) ≥126mg/dl. Impaired fasting glucose (IFG) was defined as an FPG of 100-125mg/dl. Awareness was defined as diabetes self-report, treatment as receiving glucose-lowering medications, and glycemic control as FPG <126mg/dl. The age- and sex-weighted estimates were calculated using the 2016 national census. Logistic regression models were used to determine the factors associated with diabetes awareness, treatment, and control.
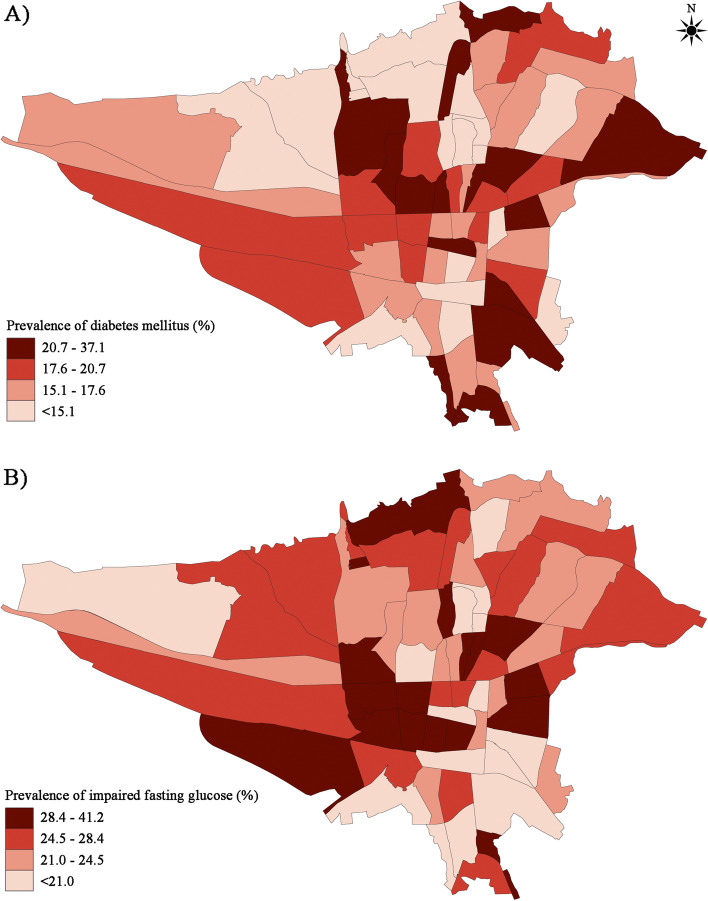
Results: A total of 8151 participants were included. Age- and sex-weighted prevalence of diabetes mellitus and IFG were 16.7% (95% CI: 15.1-18.4) and 25.1% (95% CI: 23.1-27.1), respectively. Diabetes was more prevalent in the eastern and central districts of Tehran. Advanced age (OR per 1-year increase: 1.026, 95% CI: 1.021-1.030), male sex (OR: 1.716, 95% CI: 1.543-1.909), higher BMI levels (OR for BMI ≥35 vs. <20 kg/m2: 4.852, 95% CI: 3.365-6.998), pre-existing hypertension (OR: 1.552, 95% CI: 1.378-1.747), dyslipidemia (OR: 1.692, 95% CI: 1.521-1.883), and chronic kidney disease (OR: 1.650, 95% CI: 1.019-2.673) were associated with an increased odds of diabetes mellitus. On the contrary, diabetes mellitus was less likely in current tobacco (OR: 0.872, 95% CI: 0.765-0.994) and alcohol users (OR: 0.836, 95% CI: 0.703-0.994) compared to non-users. Among diabetic individuals, 82.8% were aware of their condition, 71.9% received treatment, and 31.7% of treated patients had adequate glycemic control. Advanced age and pre-existing comorbidities, including hypertension and dyslipidemia, were associated with higher diabetes awareness and treatment. Furthermore, advanced age, higher levels of education, and female sex were determinants of better glycemic control among treated diabetic participants.
Conclusion: There is a high prevalence of diabetes and IFG among adult residents of Tehran. Additionally, more than two-thirds of treated diabetics living in Tehran remain uncontrolled.
Keywords: Awareness; Control; Diabetes mellitus; Epidemiology; Prevalence; Treatment.
© 2022. The Author(s).
Conflict of interest statement
None declared
Figures




References
-
- IDF Diabetes Atlas, 9th edition [https://www.diabetesatlas.org/en/sections/worldwide-toll-of-diabetes.html]
-
- Collaborators GBDRF Global regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1923–1994. doi: 10.1016/S0140-6736(18)32225-6. - DOI - PMC - PubMed
-
- Bagherzadeh A, Nejati-Afkham A, Tajallizade-Khoob Y, Shafiee A, Sharifi F, Esfahani MA, Badamchizade Z, Alatab S, Fakhrzadeh H. Association of cardiac autonomic neuropathy with arterial stiffness in type 2 diabetes mellitus patients. J diabetes metab disord. 2013;12(1):55. doi: 10.1186/2251-6581-12-55. - DOI - PMC - PubMed
-
- Nanayakkara N, Curtis AJ, Heritier S, Gadowski AM, Pavkov ME, Kenealy T, Owens DR, Thomas RL, Song S, Wong J, et al. Impact of age at type 2 diabetes mellitus diagnosis on mortality and vascular complications: systematic review and meta-analyses. Diabetologia. 2021;64(2):275–287. doi: 10.1007/s00125-020-05319-w. - DOI - PMC - PubMed
-
- Nanayakkara N, Ranasinha S, Gadowski AM, Davis WA, Flack JR, Wischer N, Andrikopoulos S, Zoungas S. Age-related differences in glycaemic control, cardiovascular disease risk factors and treatment in patients with type 2 diabetes: a cross-sectional study from the Australian National Diabetes Audit. BMJ Open. 2018;8(8):e020677. doi: 10.1136/bmjopen-2017-020677. - DOI - PMC - PubMed
