

Changing patterns of multidisciplinary team treatment, early mortality, and survival in colorectal cancer
- PMID: 36254731
- PMCID: PMC9577547
- DOI: 10.1093/bjsopen/zrac098
Changing patterns of multidisciplinary team treatment, early mortality, and survival in colorectal cancer
Abstract
Background: This study reports early mortality and survival from colorectal cancer in relation to the pattern of treatments delivered by the multidisciplinary team (MDT) meeting at a high-volume institution in England over 14 years.
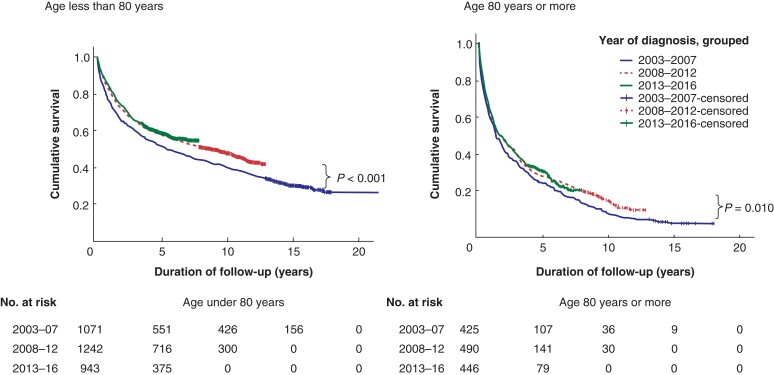
Methods: All patients diagnosed with colorectal cancer and discussed during MDT meetings from 2003 to 2016 at a single institution were reviewed. Three time intervals (2003-2007, 2008-2012, and 2013-2016) were compared regarding initial surgical management (resection, local excision, non-resection surgery, and no surgery), initial oncological therapy, 90-day mortality, and crude 2-year survival for the whole cohort. Sub-analyses were performed according to age greater or less than 80 years.
Results: The MDT managed 4617 patients over 14 years (1496 in the first interval and 1389 in the last). Over this time, there was a reduction in emergency resections from 15.5 per cent to 9.0 per cent (P < 0.0001); use of oncological therapies increased from 34.6 per cent to 41.6 per cent (P < 0.0001). The 90-day mortality after diagnosis of colorectal cancer dropped from 14.8 per cent to 10.7 per cent (P < 0.001) and 2-year survival improved from 58.6 per cent to 65 per cent (P < 0.001). Among patients aged 80 years or older (425 and 446, in the first and last intervals respectively) there was, in addition, a progressive increase in 'no surgery' rate from 33.6 per cent to 50.2 per cent (P < 0.0001) and a reduction in elective resections from 42.4 per cent to 33.9 per cent (P = 0.010). The 90-day mortality after elective resection fell from 10.0 per cent (18 of 180) to 3.3 per cent (5 of 151; P = 0.013).
Conclusions: Survival from colorectal cancer improved significantly over 14 years. Among patients aged ≥80 years, major changes in the type of treatment delivered were associated with a decrease in postoperative mortality.
© The Author(s) 2022. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures
Comment in
-
Role of frailty assessment in selection for cancer surgery.BJS Open. 2022 Sep 2;6(5):zrac117. doi: 10.1093/bjsopen/zrac117. BJS Open. 2022. PMID: 36254730 Free PMC article. No abstract available.
References
-
- Calman K, Hine D. A policy framework for commissioning cancer services: a report by the Expert Advisory Group on Cancer to the Chief Medical Officers of England and Wales. Department of Health Publications, The National Archive, 1995
-
- Liang J, Fazio V, Lavery I, Remzi F, Hull T, Strong Set al. . Primacy of surgery for colorectal cancer. Br J Surg 2015;102:847–852 - PubMed
-
- Okabe H, Ohsaki T, Ogawa K, Ozaki N, Hayashi H, Akahoshi Set al. . Frailty predicts severe postoperative complications after elective colorectal surgery. Am J Surg 2019;217:677–681 - PubMed
-
- Papamichael D, Audisio RA, Glimelius B, de Gramont A, Glynne-Jones R, Haller Det al. . Treatment of colorectal cancer in older patients: International Society of Geriatric Oncology (SIOG) consensus recommendations 2013. Ann Oncol 2015;26:463–476 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
