

Perioperative outcome of minimally invasive stabilisation of bilateral fragility fractures of the sacrum: a comparative study of bisegmental transsacral stabilisation versus spinopelvic fixation
- PMID: 36255462
- PMCID: PMC10175409
- DOI: 10.1007/s00068-022-02123-6
Perioperative outcome of minimally invasive stabilisation of bilateral fragility fractures of the sacrum: a comparative study of bisegmental transsacral stabilisation versus spinopelvic fixation
Abstract
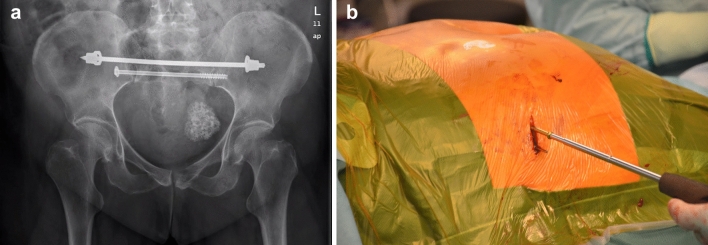
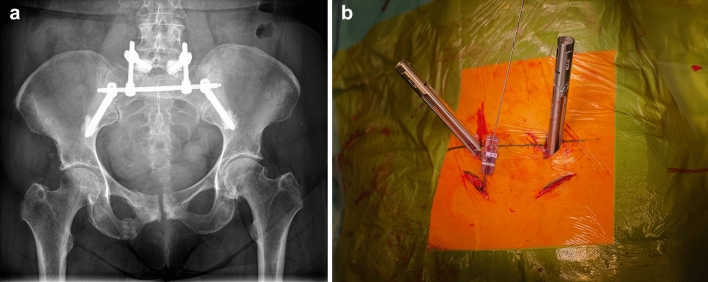
Purpose: Pelvic fragility fractures have steadily risen over the past decades. The primary treatment goal is the fastest possible mobilisation. If conservative therapy fails, surgical fixation is a promising approach. This study compares the outcome of bisegmental transsacral stabilisation (BTS) and spinopelvic fixation (SP) as minimally invasive techniques for bilateral fragility fractures of the sacrum (BFFS).
Methods: We performed a prospective, non-randomised, case-controlled study. Patients were included if they remained bedridden due to pain despite conservative treatment. Group assignment depended on sacral anatomy and fracture type. The outcome was estimated by blood loss calculation, cut-seam time, fluoroscopy time, complications, duration of stay at the intensive/intermediate care unit (ICU/IMC), and total inpatient stay. The mobility level at discharge was recorded.
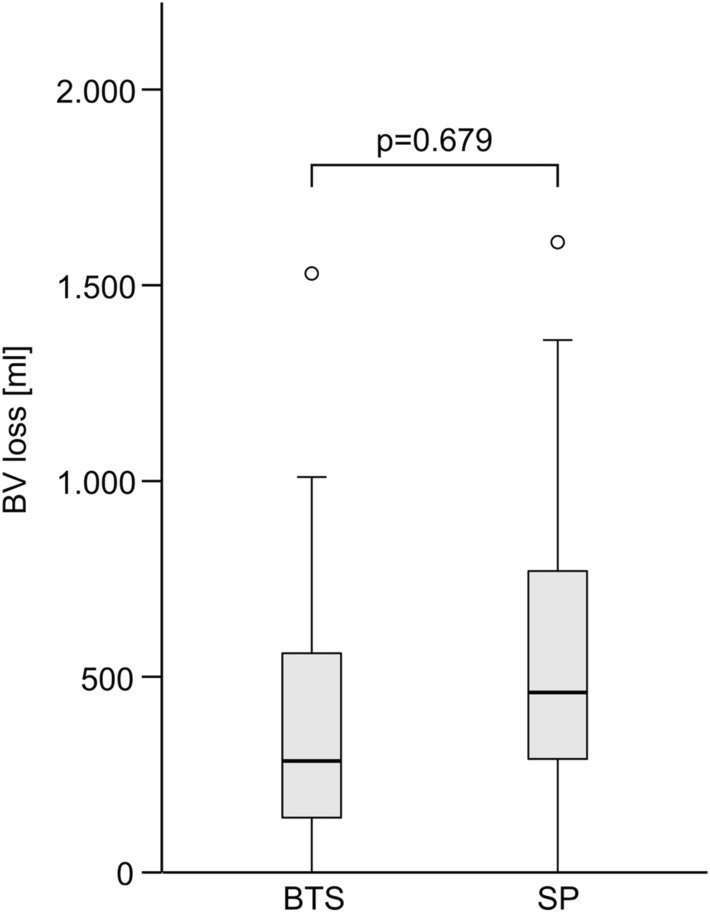
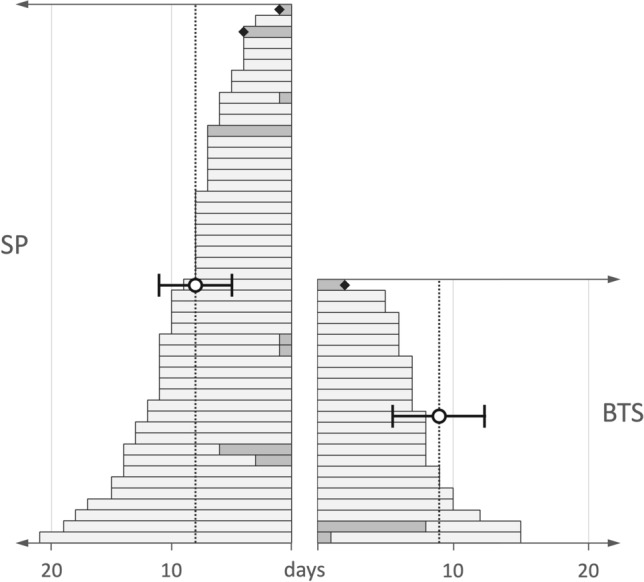
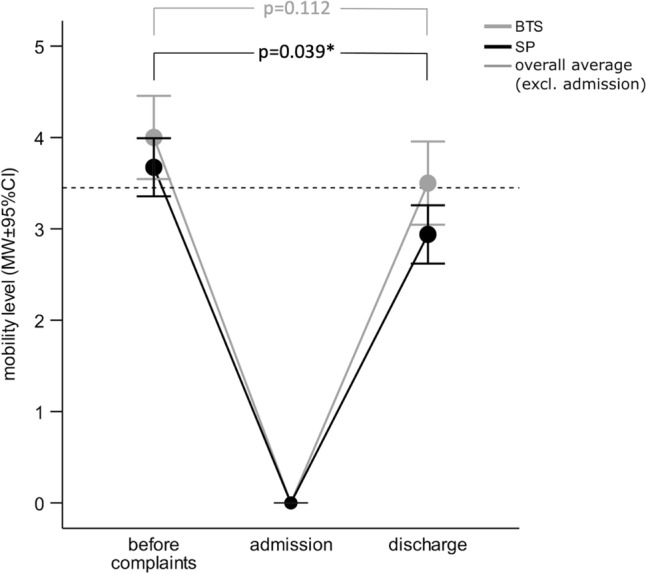
Results: Seventy-three patients were included (SP: 49, BTS: 24). There was no difference in blood loss (BTS: 461 ± 628 mL, SP: 509 ± 354 mL). BTS showed a significantly lower cut-seam time (72 ± 23 min) than SP (94 ± 27 min). Fluoroscopy time did not differ (BTS: 111 ± 61 s vs. 103 ± 45 s). Thirteen percent of BTS and 16% of SP patients required ICU/IMC stay (BTS: 0.6 ± 1.8 days, SP: 0.5 ± 1.5 days) during inpatient stay (BTS: 9 ± 4 days, SP: 8 ± 3 days). Fourteen patients suffered from urinary tract infections (BTS: 8%; SP: 25%). In-patient mortality was low (BTS: 4.2%, SP: 4.1%). At discharge, the BTS group was almost back to the initial mobility level. In SP patients, mobility was significantly lower than before complaints (p = 0.004).
Conclusion: Both methods allow early mobilization of BFFS patients. Blood loss can be kept low. Hence, transfusion requirement is correspondingly low. The IMC/ICU and the total inpatient stay are lower than reported in the literature. Both BTS and SP can be recommended as safe and low-complication methods for use in BFFS patients. BTS is superior to SP with respect to surgery duration and level of mobility at discharge.
Keywords: Bilateral fragility fracture of the sacrum; Bisegmental transsacral stabilization; Blood loss; Complications; Fragility fracture of the pelvis; Geriatric; Short-term outcome; Spinopelvic fixation.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

Similar articles
-
Mid-term outcome of bilateral fragility fractures of the sacrum after bisegmental transsacral stabilization versus spinopelvic fixation.Bone Joint J. 2021 Mar;103-B(3):462-468. doi: 10.1302/0301-620X.103B3.BJJ-2020-1454.R1. Bone Joint J. 2021. PMID: 33641427
-
The surgical management of highly unstable fragility fractures of the sacrum with spinopelvic dissociation: A case series and proposal of a surgical treatment algorithm.Injury. 2022 Oct;53(10):3377-3383. doi: 10.1016/j.injury.2022.08.031. Epub 2022 Aug 18. Injury. 2022. PMID: 36028371
-
[Minimally invasive stabilization of fragility fractures of the pelvis with transsacral bar and retrograde transpubic screw].Oper Orthop Traumatol. 2022 Apr;34(2):153-171. doi: 10.1007/s00064-022-00763-w. Epub 2022 Mar 17. Oper Orthop Traumatol. 2022. PMID: 35301551 German.
-
2D versus 3D fluoroscopy-based navigation in posterior pelvic fixation: review of the literature on current technology.Int J Comput Assist Radiol Surg. 2017 Jan;12(1):69-76. doi: 10.1007/s11548-016-1465-5. Epub 2016 Aug 8. Int J Comput Assist Radiol Surg. 2017. PMID: 27503119 Review.
-
Posterior pelvic ring injuries, lumbosacral junction instabilities and stabilization techniques for spinopelvic dissociation: a narrative review.Arch Orthop Trauma Surg. 2024 Apr;144(4):1627-1635. doi: 10.1007/s00402-024-05211-x. Epub 2024 Feb 14. Arch Orthop Trauma Surg. 2024. PMID: 38353686 Review.
Cited by
-
Compressive effect and collapse behavior of three different transsacral implants in sacral fragility fractures - a retrospective analysis of 106 cases.Eur J Trauma Emerg Surg. 2024 Dec;50(6):2963-2973. doi: 10.1007/s00068-024-02629-1. Epub 2024 Aug 27. Eur J Trauma Emerg Surg. 2024. PMID: 39190062 Free PMC article.
-
Transiliac-Transsacral Screw Fixation is Superior to Lumbopelvic Stabilization in the Treatment of Minimally Displaced Sacral H-/U-Type Fragility Fractures.Global Spine J. 2025 May;15(4):1939-1949. doi: 10.1177/21925682241268141. Epub 2024 Jul 26. Global Spine J. 2025. PMID: 39058691 Free PMC article.
-
[Sacral H-shaped fractures between traumatic, insufficiency and fatigue fractures : Similarities, differences and controversies].Unfallchirurgie (Heidelb). 2023 Nov;126(11):863-871. doi: 10.1007/s00113-023-01346-5. Epub 2023 Jul 4. Unfallchirurgie (Heidelb). 2023. PMID: 37401983 Review. German.
References
-
- Mendel T, Ullrich BW, Hofmann GO, Schenk P, Goehre F, Schwan S, Klauke F. Progressive instability of bilateral sacral fragility fractures in osteoporotic bone: a retrospective analysis of X-ray, CT, and MRI datasets from 78 cases. Eur J Trauma Emerg Surg. 2020 doi: 10.1007/s00068-020-01480-4. - DOI - PubMed
-
- Mendel T, Schenk P, Ullrich BW, Hofmann GO, Goehre F, Schwan S, et al. Mid-term outcome of bilateral fragility fractures of the sacrum after bisegmental transsacral stabilization versus spinopelvic fixation. Bone Jt J. 2021;103-B(3):462–468. doi: 10.1302/0301-620X.103B3.BJJ-2020-1454.R1. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
