

Vestibular paroxysmia entails vestibular nerve function, microstructure and endolymphatic space changes linked to root-entry zone neurovascular compression
- PMID: 36255522
- PMCID: PMC9813125
- DOI: 10.1007/s00415-022-11399-y
Vestibular paroxysmia entails vestibular nerve function, microstructure and endolymphatic space changes linked to root-entry zone neurovascular compression
Abstract
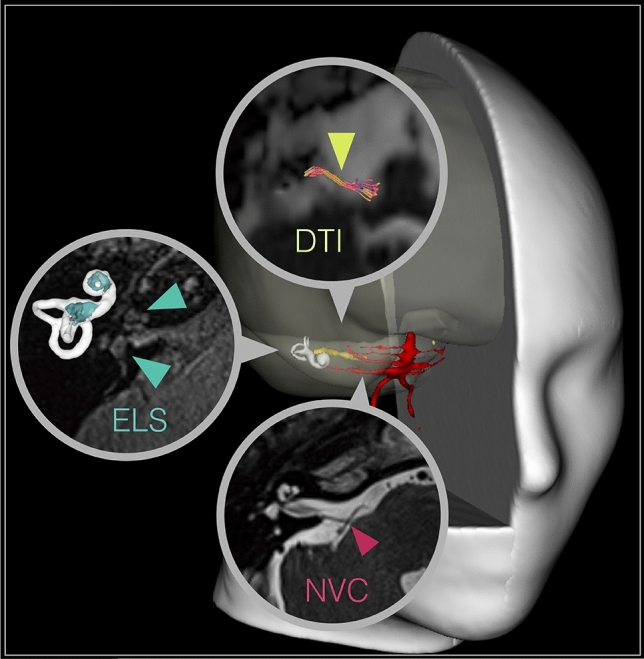
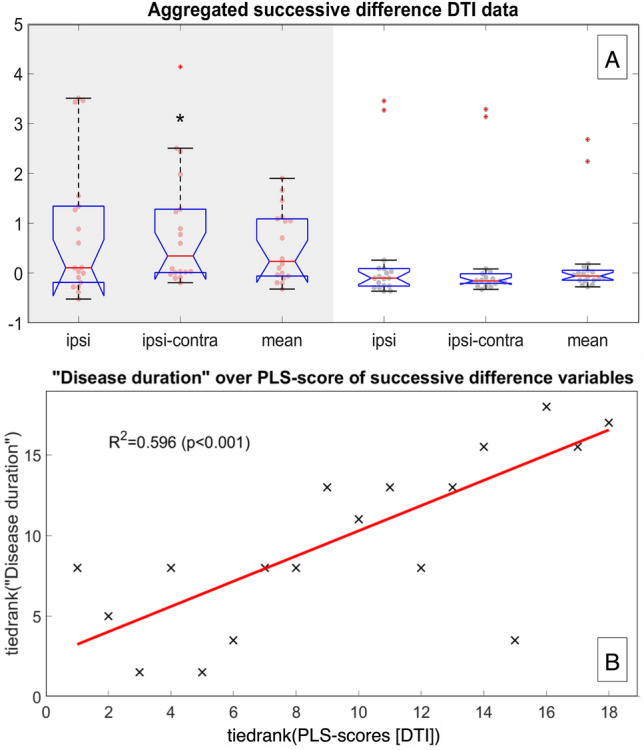
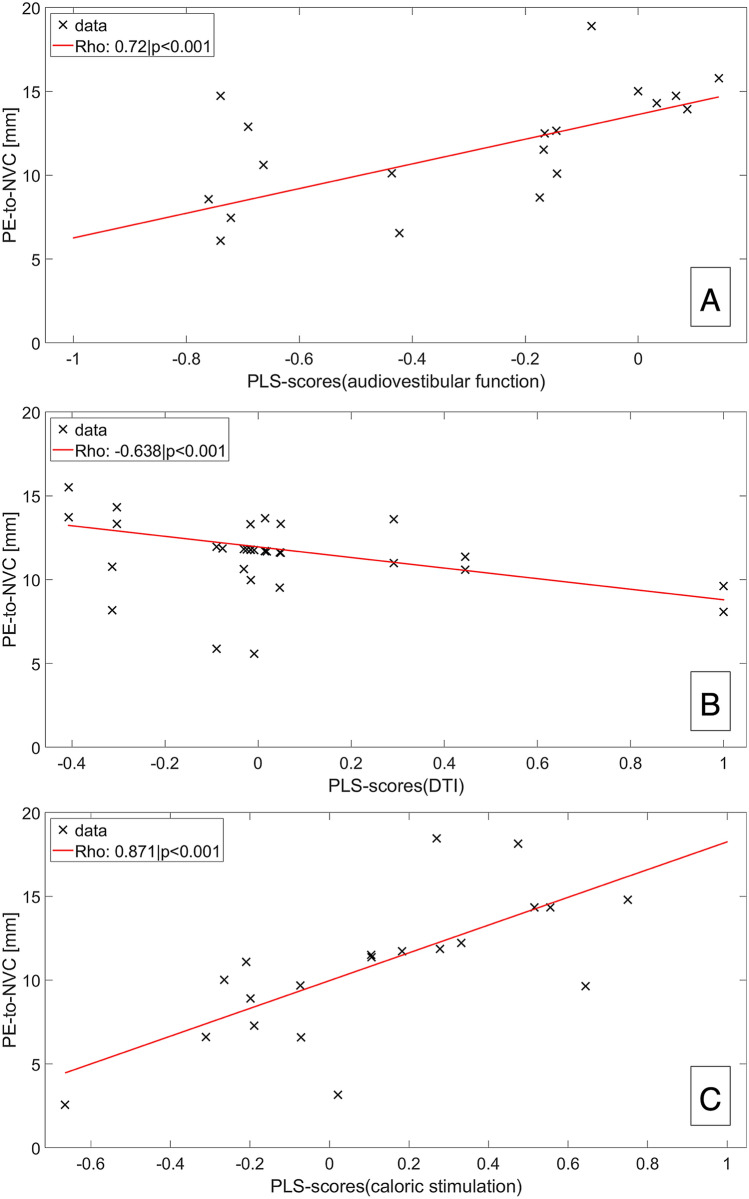
Combining magnetic resonance imaging (MRI) sequences that permit the determination of vestibular nerve angulation (NA = change of nerve caliber or direction), structural nerve integrity via diffusion tensor imaging (DTI), and exclusion of endolymphatic hydrops (ELH) via delayed gadolinium-enhanced MRI of the inner ear (iMRI) could increase the diagnostic accuracy in patients with vestibular paroxysmia (VP). Thirty-six participants were examined, 18 with VP (52.6 ± 18.1 years) and 18 age-matched with normal vestibulocochlear testing (NP 50.3 ± 16.5 years). This study investigated whether (i) NA, (ii) DTI changes, or (iii) ELH occur in VP, and (iv) to what extent said parameters relate. Methods included vestibulocochlear testing and MRI data analyses for neurovascular compression (NVC) and NA verification, DTI and ELS quantification. As a result, (i) NA increased NVC specificity. (ii) DTI structural integrity was reduced on the side affected by VP (p < 0.05). (iii) 61.1% VP showed mild ELH and higher asymmetry indices than NP (p > 0.05). (iv) "Disease duration" and "total number of attacks" correlated with the decreased structural integrity of the affected nerve in DTI (p < 0.001). NVC distance within the nerve's root-entry zone correlated with nerve function (Roh = 0.72, p < 0.001), nerve integrity loss (Roh = - 0.638, p < 0.001), and ELS volume (Roh = - 0.604, p < 0.001) in VP. In conclusion, this study is the first to link eighth cranial nerve function, microstructure, and ELS changes in VP to clinical features and increased vulnerability of NVC in the root-entry zone. Combined MRI with NVC or NA verification, DTI and ELS quantification increased the diagnostic accuracy at group-level but did not suffice to diagnose VP on a single-subject level due to individual variability and lack of diagnostic specificity.
Keywords: DTI; Diffusion imaging; Endolymphatic hydrops; Endolymphatic space; Gadolinium-based contrast agent; Inner ear; Intravenous; MRI; Root-entry zone; Vestibular nerve; Vestibular paroxysmia.
© 2022. The Author(s).
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Brandt T, Dieterich M, Strupp M. Vertigo and dizziness: common complaints. 2. London: Springer-Verlag; 2013.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
