

Coadministration of seasonal influenza and COVID-19 vaccines: A systematic review of clinical studies
- PMID: 36256633
- PMCID: PMC9746457
- DOI: 10.1080/21645515.2022.2131166
Coadministration of seasonal influenza and COVID-19 vaccines: A systematic review of clinical studies
Abstract
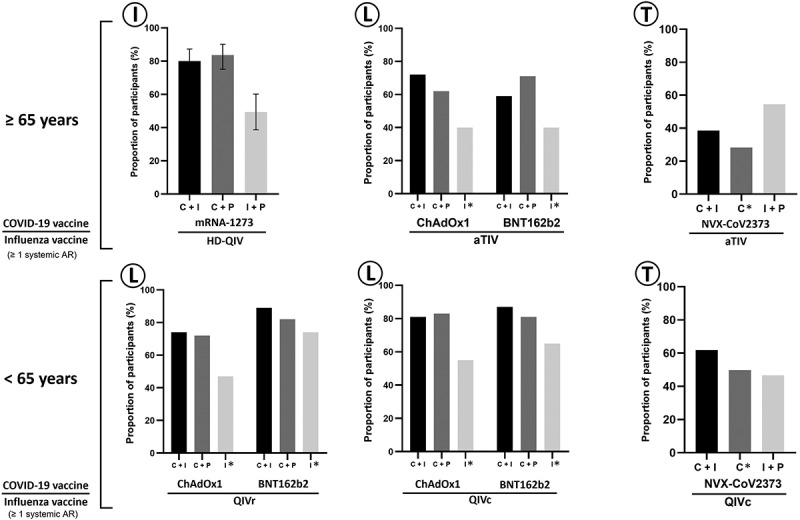
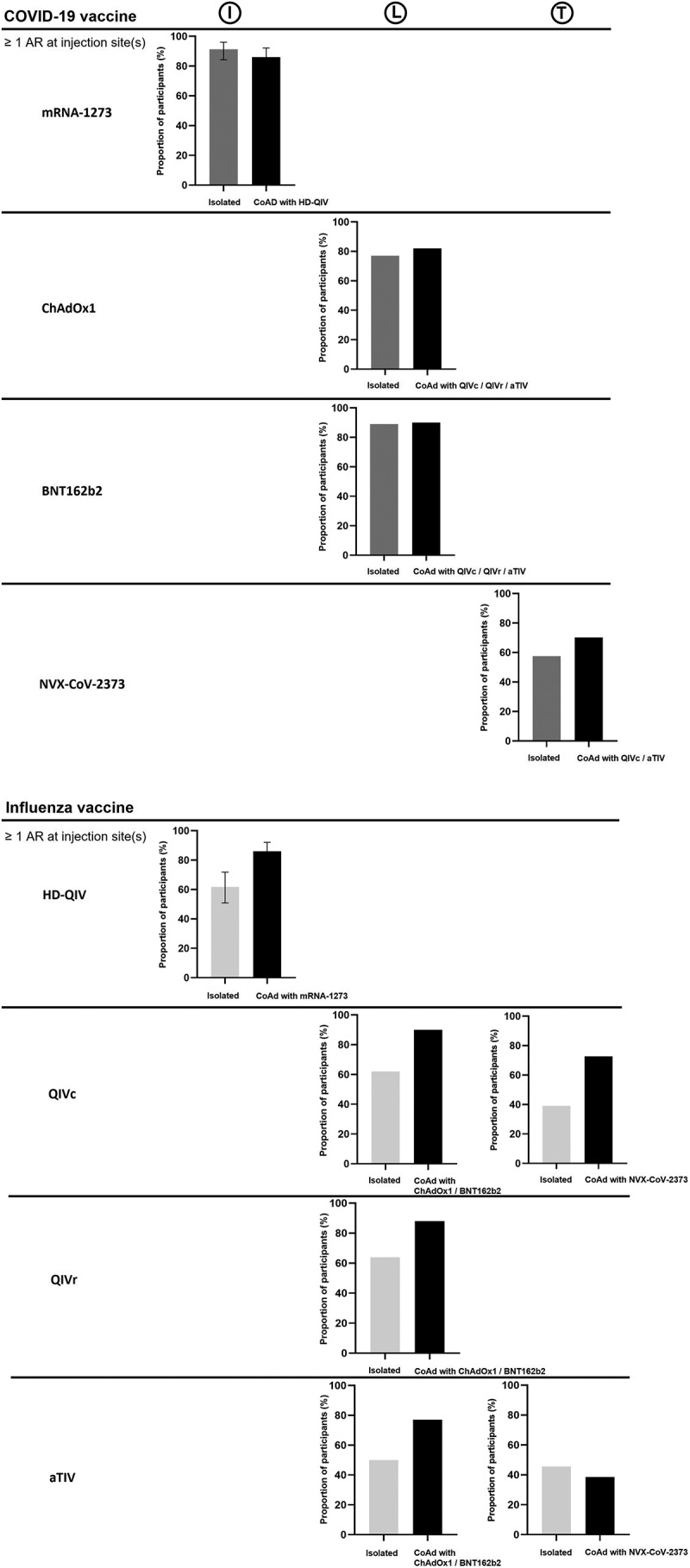
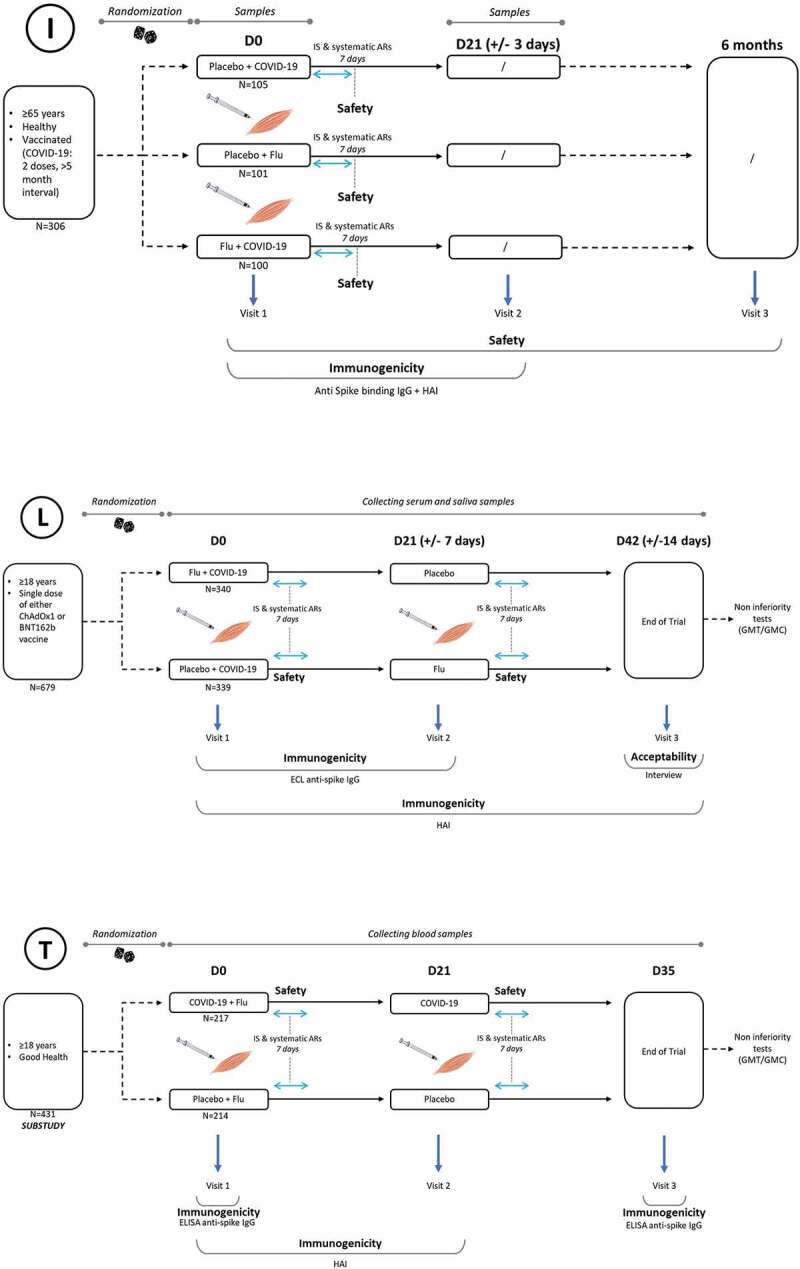
The lifting of non-pharmaceutical measures preventing transmission of SARS-CoV-2 (and other viruses, including influenza viruses) raises concerns about healthcare resources and fears of an increased number of cases of influenza and COVID-19. For the 2021-2022 influenza season, the WHO and >20 European countries promoted coadministration of influenza and COVID-19 vaccines. Recently, the French Health Authority recommended coupling the COVID-19 vaccination with the 2022-2023 influenza vaccination campaign for healthcare professionals and people at risk of severe COVID-19. The present systematic review examines published data on the safety, immunogenicity, efficacy/effectiveness, and acceptability/acceptance of coadministration of influenza and COVID-19 vaccines. No safety concerns or immune interferences were found whatever the vaccines or the age of vaccinated subjects (65- or 65+). No efficacy/effectiveness data were available. The results should reassure vaccinees and vaccinators in case of coadministration and increase vaccine coverage. Healthcare systems promoting coupled campaigns must provide the necessary means for successful coadministration.
Keywords: COVID-19 vaccines; Coadministration; influenza vaccines; patient acceptance of healthcare; patient compliance; patient safety; vaccine efficacy; vaccine immunogenicity.
Plain language summary
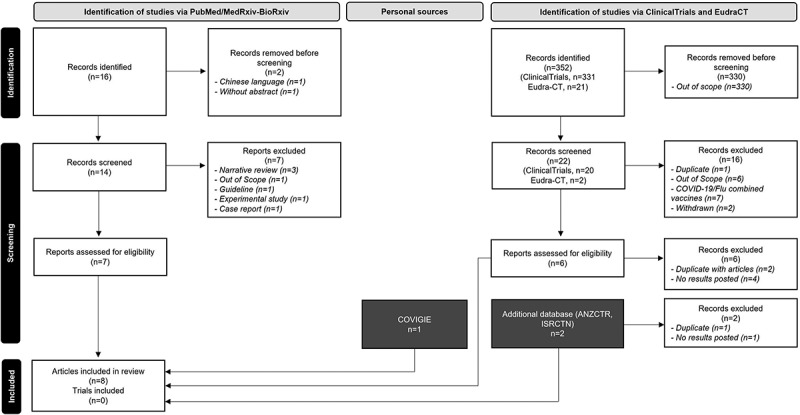
The lifting of non-pharmaceutical measures recommended to prevent transmission of SARS-CoV-2 (and other viruses, including influenza viruses) raises concerns about healthcare resources, already under pressure. It also raises fears of an increase in the number of cases of influenza or COVID-19 infection during the winter season. For the 2021–2022 influenza season, the World Health Organization and several European countries promoted concomitant administration in distinct anatomic sites (i.e., coadministration) of influenza and COVID-19 vaccines to avoid additional stress on healthcare systems. In May 2022, the French Health Authority recommended coupling the COVID-19 vaccination with the 2022–2023 influenza vaccination campaign (i.e., starting COVID-19 vaccination at the date of influenza vaccination) for healthcare professionals and people at risk of severe COVID-19, in case of epidemic wave. Coadministration of influenza and COVID-19 vaccines is one of the factors of success for a coupled campaign. The present systematic review examines all published data (articles or reports, clinical trials, or surveys) on the safety, immunogenicity, efficacy/effectiveness, and acceptability/acceptance of coadministration of influenza and COVID-19 vaccines. The PRISMA method was used to collect information. No safety concerns or immune interferences were found whatever the vaccines or the age of vaccinated subjects (65- or 65+). No efficacy/effectiveness data were available. Acceptability and acceptance were good but could be improved. By reassuring vaccinees and vaccinators, these results are expected to favor coadministration and ultimately increase vaccine coverage, thus offering better protection. Healthcare systems promoting coupled campaigns with coadministration must provide the necessary means for their successful implementation.
Conflict of interest statement
C.J. reports fees for board membership from AstraZeneca, Pfizer, Sanofi and MSD, consultant and speaker for these companies, participation in congresses on invitation by these companies.
A.M. reports to participate in an advisory committee organized by Sanofi and to be a member of the scientific board of the GEIG and the scientific board of the POSTHER study (Herpes Zoster Study, GSK).
G.G. reports to participate in advisory committees organized by Astellas, AstraZeneca, BioMérieux, MSD, Pfizer, Sanofi, Sanofi Pasteur, Sanofi Pasteur-MSD and Vifor, consultant and speaker for these companies, participation in congresses on invitation by Eisai, MSD, Novartis, Pfizer, Sanofi, and Vifor.
B.C. reports to participate in advisory board organized by AstraZeneca, Sanofi and Osivax and to participate to conferences on invitation by Pfizer and GSK.
P.C. reports to participate in advisory committees organized by Sanofi and being consultant for Sanofi.
J.G. reports to participate in advisory committees organized by GSK, MSD, Pfizer, and Sanofi.
O.L. reports to be principal investigator in vaccine trials sponsored by Sanofi, MSD, Pfizer, GSK, Moderna. She received financial support for traveling to medical congress and personal fees for participation to advisory boards for Sanofi, MSD, Pfizer, and GSK.
E.B.-N. conducts vaccine trials including COVID-19 trials using Janssen, Pfizer, Moderna, and Sanofi COVID-19 vaccines. She participated in vaccines scientific advisory boards for Pfizer, Janssen, and Sanofi with honoraria paid to her institution.
Figures
References
-
- WHO, World Health Organization . Vaccines against influenza: wHO position paper. Weekly Epidemiological Record. 2022. May 13 [accessed 2022 Jun 21]. https://www.who.int/publications-detail-redirect/who-wer9719-185-208.
-
- Melidou A, Ködmön C, Nahapetyan K, Kraus A, Alm E, Adlhoch C, Mooks P, Dave N, Carvalho C, Meslé M, et al. Influenza returns with a season dominated by clade 3c.2a1b.2a.2 A(H3N2) viruses, WHO European region, 2021/22. Euro Surveill. 2022;27(15):1. PII: 2200255. doi: 10.2807/1560-7917.ES.2022.27.15.2200255. - DOI - PMC - PubMed
-
- Australian Government Department of health . Australian influenza surveillance report - No 05 - fortnight ending 05 June 2022. Australia: Australian Government Department of Health; 2022. Report No: 05.
-
- Li Y, Campbell H, Kulkarni D, Harpur A, Nundy M, Wang X, Nair H.. The temporal association of introducing and lifting non-pharmaceutical interventions with the time-varying reproduction number (R) of SARS-CoV-2: a modelling study across 131 countries. Lancet Infect Dis. 2021;21(2):193–12. doi: 10.1016/S1473-3099(20)30785-4. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous