

Impact of a diverting ileostomy in total mesorectal excision with primary anastomosis for rectal cancer
- PMID: 36258000
- PMCID: PMC10017638
- DOI: 10.1007/s00464-022-09669-x
Impact of a diverting ileostomy in total mesorectal excision with primary anastomosis for rectal cancer
Abstract
Background: The role of diverting ileostomy in total mesorectal excision (TME) for rectal cancer with primary anastomosis is debated. The aim of this study is to gain insight in the clinical consequences of a diverting ileostomy, with respect to stoma rate at one year and stoma-related morbidity.
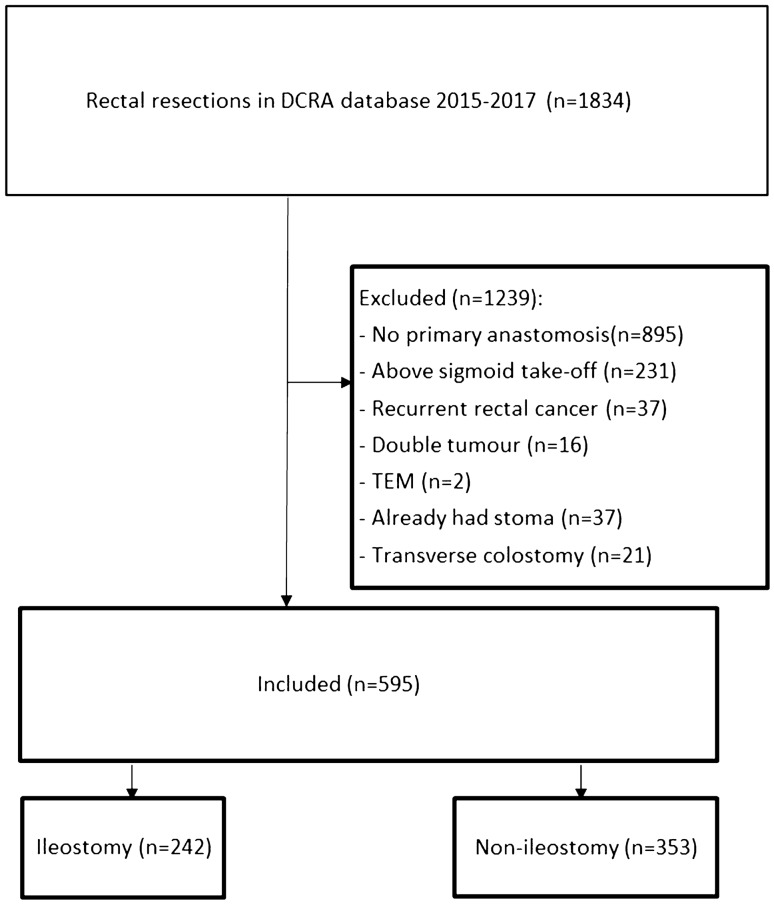
Methods: Patients undergoing TME with primary anastomosis for rectal cancer between 2015 and 2017 in eleven participating hospitals were included. Retrospectively, two groups were compared: patients with or without diverting ileostomy construction during primary surgery. Primary endpoint was stoma rate at one year. Secondary endpoints were severity and rate of anastomotic leakage, overall morbidity rate within thirty days and stoma (reversal) related morbidity.
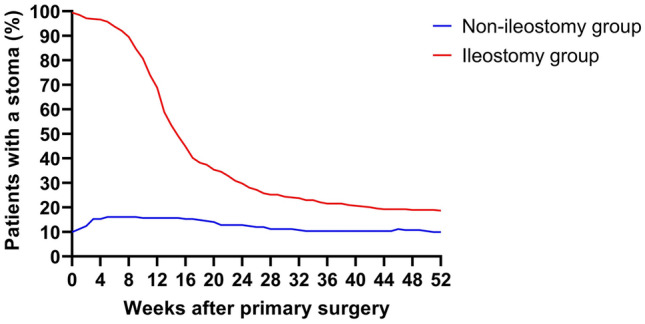
Results: In 353 out of 595 patients (59.3%) a diverting ileostomy was constructed during primary surgery. Stoma rate at one year was 9.9% in the non-ileostomy group and 18.7% in the ileostomy group (p = 0.003). After correction for confounders, multivariate analysis showed that the construction of a diverting ileostomy during primary surgery was an independent risk factor for stoma at one year (OR 2.563 (95%CI 1.424-4.611), p = 0.002). Anastomotic leakage rate was 17.8% in the non-ileostomy group and 17.2% in the ileostomy group (p = 0.913). Overall 30-days morbidity rate was 37.6% in the non-ileostomy group and 56.1% in the ileostomy group (p < 0.001). Stoma reversal related morbidity rate was 17.9%.
Conclusions: The stoma rate at one year was higher in patients with ileostomy construction during primary surgery. The incidence and severity of anastomotic leakage were not reduced by construction of an ileostomy. The morbidity related to the presence and reversal of a diverting ileostomy was substantial.
Keywords: Ileostomy; Laparoscopy; Rectal cancer.
© 2022. The Author(s).
Conflict of interest statement
Rogier M.P.H. Crolla and Esther C.J. Consten received fees for proctoring from Intuitive Surgical. Colin Sietses received surgical lecturing fees from Medtronic. For the remaining authors (Jeroen C. Hol, Thijs A. Burghgraef, Marieke L.W. Rutgers, Anna A.W. van Geloven, Gabie M. de Jong, Roel Hompes, Jeroen W.A. Leijtens, Fatih Polat, Apollo Pronk, Anke B. Smits, Jurriaan B. Tuynman, Emiel G.G. Verdaasdonk) no conflicts of interests were declared. No funding was received for this study.
Figures
References
-
- Heald RJ, Husband EM, Ryall RD. The mesorectum in rectal cancer surgery–the clue to pelvic recurrence? Br J Surg. 1982;69(10):613–616. - PubMed
-
- Bonjer HJ, Deijen CL, Haglind E, et al. A Randomized trial of laparoscopic versus open surgery for rectal cancer. N Engl J Med. 2015;373(2):194. - PubMed
-
- van der Pas MH, Haglind E, Cuesta MA, et al. Laparoscopic versus open surgery for rectal cancer (COLOR II): short-term outcomes of a randomised, phase 3 trial. Lancet Oncol. 2013;14(3):210–218. - PubMed
-
- Stevenson AR, Solomon MJ, Lumley JW, et al. Effect of Laparoscopic-Assisted Resection vs Open Resection on Pathological Outcomes in Rectal Cancer: The ALaCaRT Randomized Clinical Trial. JAMA. 2015;314(13):1356–1363. - PubMed
-
- McDermott FD, Heeney A, Kelly ME, et al. Systematic review of preoperative, intraoperative and postoperative risk factors for colorectal anastomotic leaks. Br J Surg. 2015;102(5):462–479. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
