

IMproving PULmonary hypertension Screening by Echocardiography: IMPULSE
- PMID: 36258244
- PMCID: PMC9580132
- DOI: 10.1186/s44156-022-00010-9
IMproving PULmonary hypertension Screening by Echocardiography: IMPULSE
Abstract
Background: The world symposium on pulmonary hypertension (PH) has proposed that PH be defined as a mean pulmonary artery pressure (mPAP) > 20 mmHg as assessed by right heart catheterisation (RHC). Transthoracic echocardiography (TTE) is an established screening tool used for suspected PH. International guidelines recommend a multi-parameter assessment of the TTE PH probability although effectiveness has not been established using real world data.
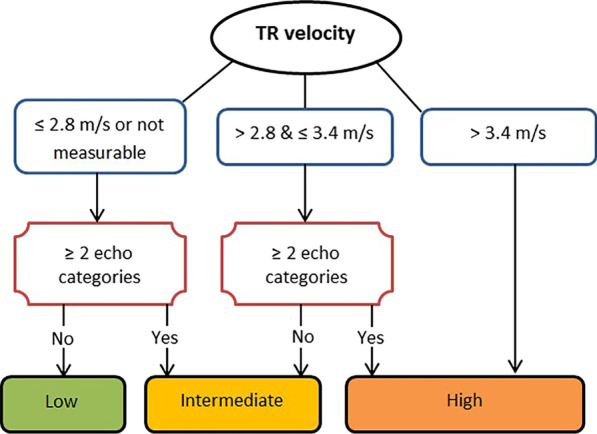
Study aims: To determine accuracy of the European Society of Cardiology (ESC) and British Society of Echocardiography (BSE) TTE probability algorithm in detecting PH in patients attending a UK PH centre. To identify echocardiographic markers and revised algorithms to improve the detection of PH in those with low/intermediate BSE/ESC TTE PH probability.
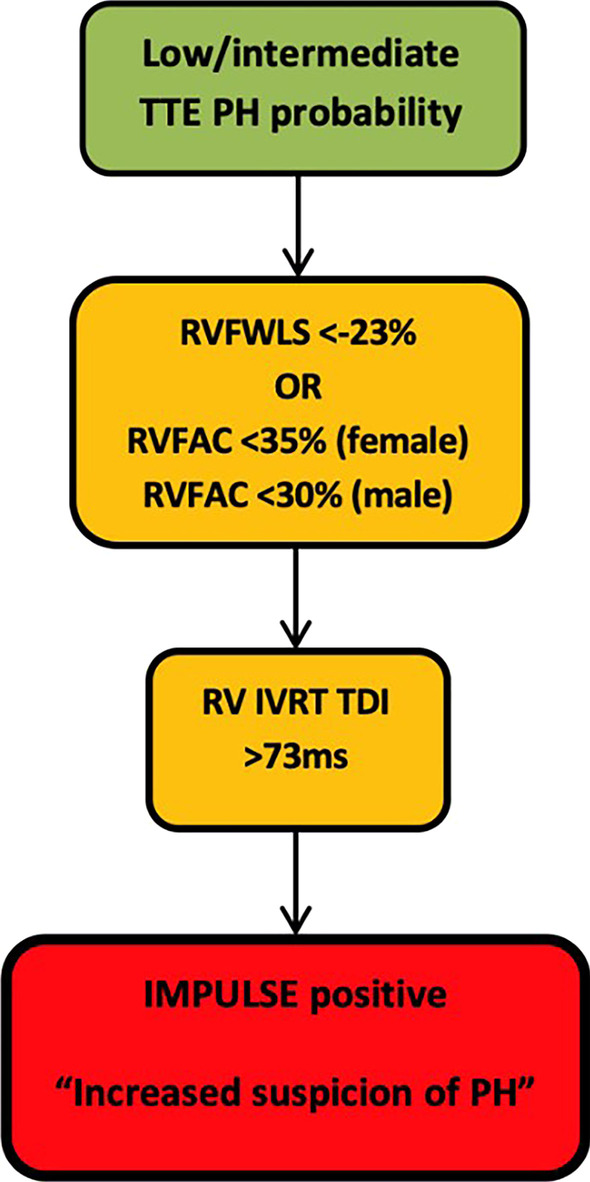
Methods: TTE followed by RHC (within 4 months after) was undertaken in patients for suspected but previously unconfirmed PH. BSE/ESC PH TTE probabilities were calculated alongside additional markers of right ventricular (RV) longitudinal and radial function, and RV diastolic function. A refined IMPULSE algorithm was devised and evaluated in patients with low and/or intermediate ESC/BSE TTE PH probability.
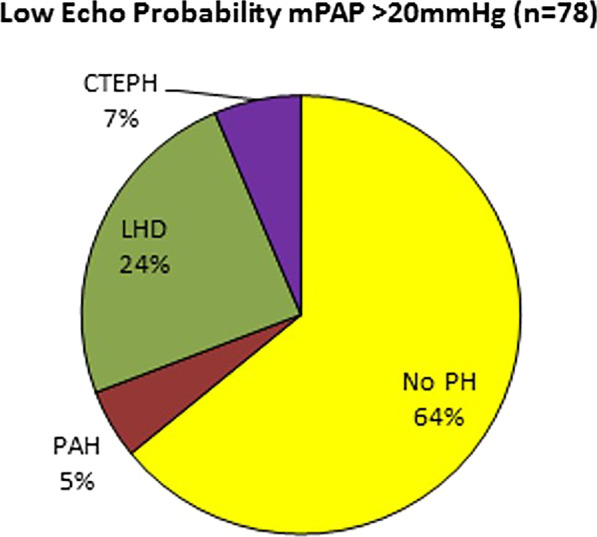
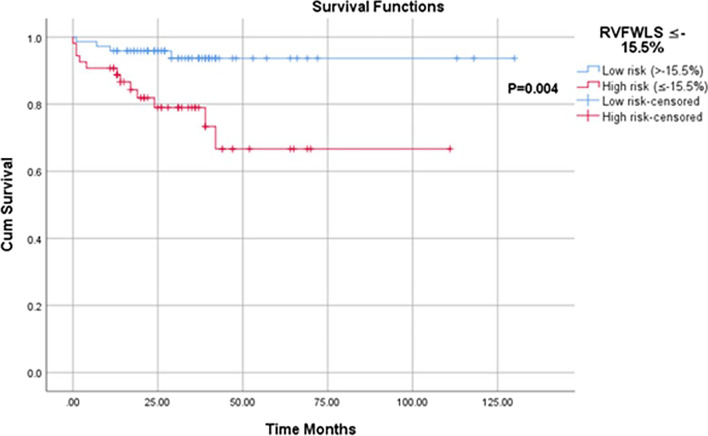
Results: Of 310 patients assessed, 236 (76%) had RHC-confirmed PH (average mPAP 42.8 ± 11.7). Sensitivity and specificity for detecting PH using the BSE/ESC recommendations was 89% and 68%, respectively. 36% of those with low BSE/ESC TTE probability had RHC-confirmed PH and BSE/ESC PH probability parameters did not differ amongst those with and without PH in the low probability group. Conversely, RV free wall longitudinal strain (RVFWLS) was lower in patients with vs. without PH in low BSE/ESC probability group (- 20.6 ± 4.1% vs - 23.8 ± 3.9%) (P < 0.02). Incorporating RVFWLS and TTE features of RV radial and diastolic function (RVFAC and IVRT) within the IMPULSE algorithm reduced false negatives in patients with low BSE/ESC PH probability by 29%. The IMPULSE algorithm had excellent specificity and positive predictive value in those with low (93%/80%, respectively) or intermediate (82%/86%, respectively) PH probability.
Conclusion: Existing TTE PH probability guidelines lack sensitivity to detect patients with milder haemodynamic forms of PH. Combining additional TTE makers assessing RV radial, longitudinal and diastolic function enhance identification of milder forms of PH, particularly in those who have a low BSE/ESC TTE PH probability.
Keywords: Echocardiography; Pulmonary hypertension; RV free wall longitudinal strain.
© 2022. The Author(s).
Conflict of interest statement
None.
Figures
References
-
- Hoeper MM, Kramer T, Pan Z, Eichstaedt CA, Spiesshoefer J, Benjamin N, Olsson KM, et al. Mortality in pulmonary arterial hypertension: prediction by the 2015 European pulmonary hypertension guidelines risk stratification model. Eur Respir J. 2017;50(2):1700740. doi: 10.1183/13993003.00740-2017. - DOI - PubMed
-
- Galie N, Humbert M, Vachiery J, Gibbs S, Lang I, Torbicki A, Simonneau G, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS) Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT) Eur Heart J. 2016;37(1):67–119. doi: 10.1093/eurheartj/ehv317. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
