

A rare cause of abdominal pain managed unconventionally: acute renal infarction caused by atrial fibrillation: a case report
- PMID: 36258245
- PMCID: PMC9580199
- DOI: 10.1186/s13256-022-03608-z
A rare cause of abdominal pain managed unconventionally: acute renal infarction caused by atrial fibrillation: a case report
Abstract
Background: Atrial fibrillation is one of the most common arrhythmias. The main thrombotic complication of arterial fibrillation is ischemic stroke, but it can also cause acute renal infarction from embolization. The low incidence and nonspecific clinical manifestations of acute renal infarction make it difficult to diagnose, often leading to either delayed diagnosis or misdiagnosis. Due to its rarity, more efficient treatment guidelines are helpful for the management of acute renal infarction related to the thromboembolic complication of arterial fibrillation.
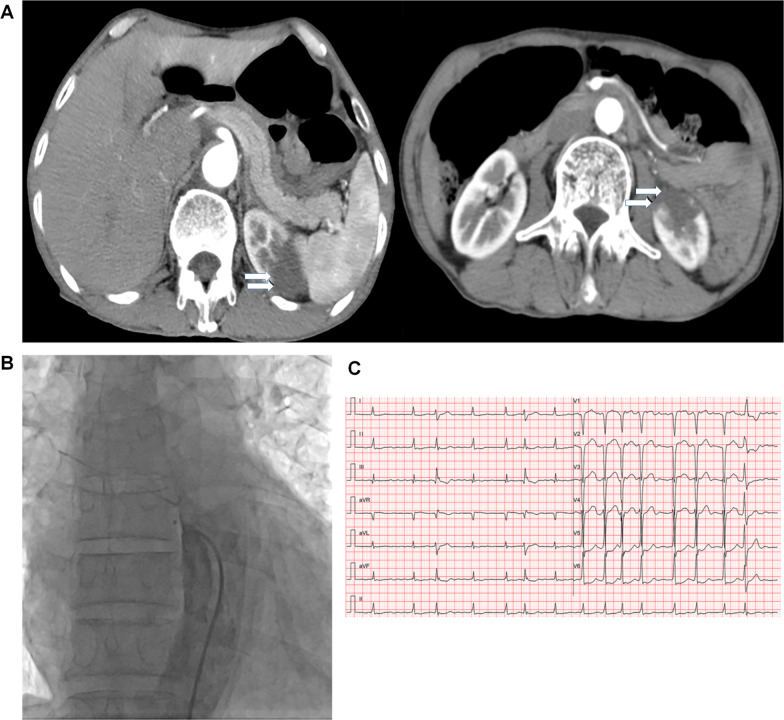
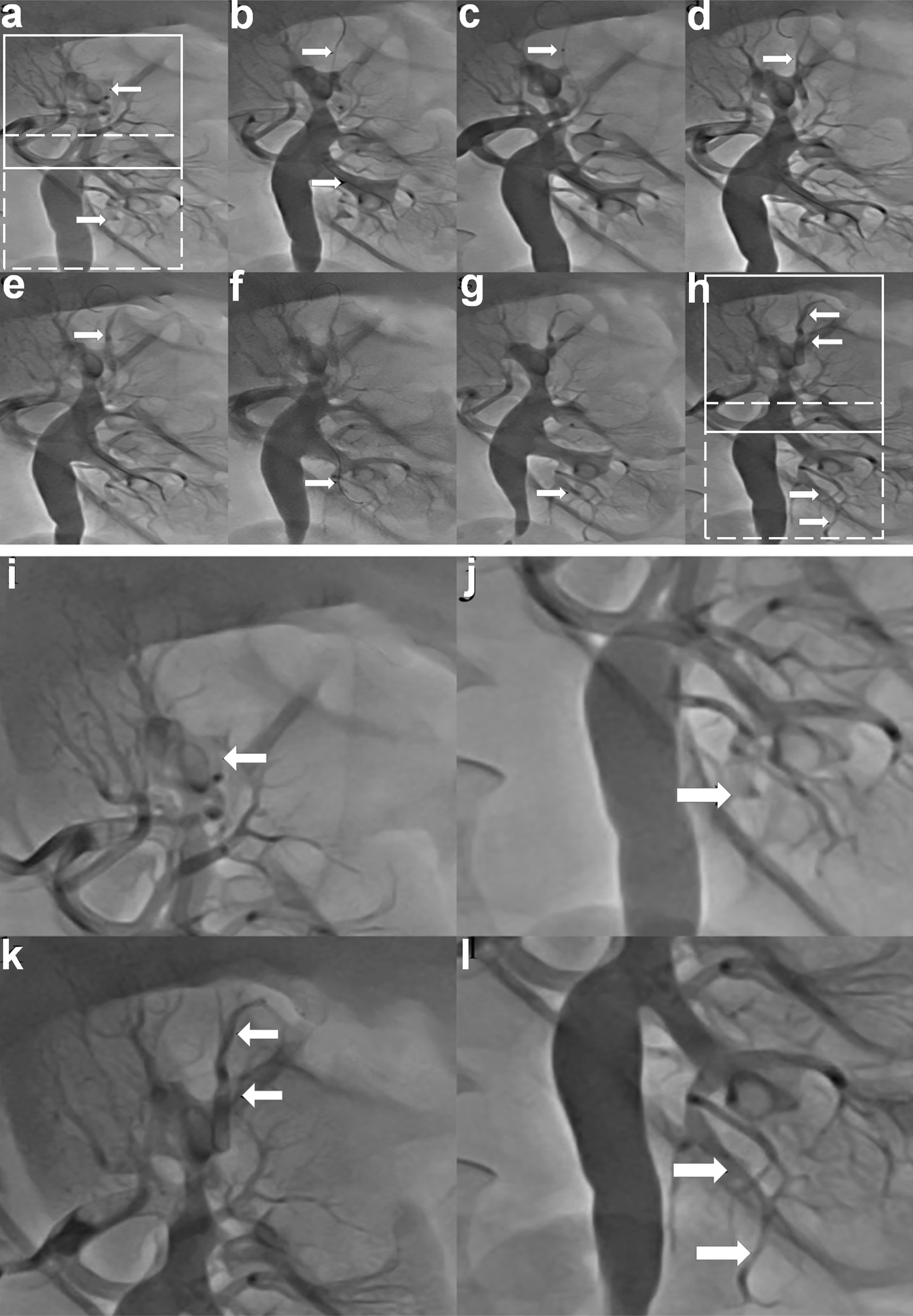
Case reports: We report a case of acute renal infarction due to underlying arterial fibrillation, where a novel interventional therapeutic method was used. A 66-year-old Chinese man with arterial fibrillation, not on anticoagulation due to the patient's preference, and coronary artery disease post-percutaneous coronary intervention to left anterior descending artery about 1 year ago, was currently on dual antiplatelet therapy. He suddenly developed intermittent and sharp left-sided abdominal pain and was found to have an acute left renal infarction on computed tomography scan. Angiogram showed acute occlusion of the left renal artery due to thromboembolism. For this patient, a combination method of local thrombus aspiration, angioplasty, and infusion of nitroglycerin and diltiazem were used, restoring blood flow to the left kidney. After recovery, the patient was discharged on aspirin, clopidogrel, and warfarin. At 6 months follow-up, there was no residual kidney dysfunction.
Conclusions: Acute renal infarction from thromboembolism is a rare but serious complication of arterial fibrillation. More efficient and different options for intervention methods will benefit the treatment of this disease. Here, we report a combination therapeutic method that has not been used in acute renal infarction associated with arterial fibrillation, and which restored renal perfusion and prevented long-term kidney injury.
Keywords: Abdominal pain; Acute renal infarction; Atrial fibrillation; Interventional therapy.
© 2022. The Author(s).
Conflict of interest statement
All authors declared that no financial and personal relationships with other people or organizations could inappropriately influence (bias) their work.
Figures
Similar articles
-
Acute Myocardial Infarction Due to Coronary Artery Embolism in a 22-Year-Old Woman with Mitral Stenosis with Atrial Fibrillation Under Warfarinization: Successful Management with Anticoagulation.Am J Case Rep. 2017 Apr 7;18:361-366. doi: 10.12659/ajcr.902250. Am J Case Rep. 2017. PMID: 28386054 Free PMC article.
-
Effect of Lesion Complexity and Clinical Risk Factors on the Efficacy and Safety of Dabigatran Dual Therapy Versus Warfarin Triple Therapy in Atrial Fibrillation After Percutaneous Coronary Intervention: A Subgroup Analysis From the REDUAL PCI Trial.Circ Cardiovasc Interv. 2020 Apr;13(4):e008349. doi: 10.1161/CIRCINTERVENTIONS.119.008349. Epub 2020 Apr 7. Circ Cardiovasc Interv. 2020. PMID: 32252548 Clinical Trial.
-
Acute myocardial infarction and arterial embolism in a patient with newly diagnosed renal mass: management dilemmas! A case report.BMC Urol. 2021 Aug 18;21(1):111. doi: 10.1186/s12894-021-00870-z. BMC Urol. 2021. PMID: 34407783 Free PMC article.
-
Managing antithrombotic therapy in patients with both atrial fibrillation and coronary heart disease.Clin Ther. 2014 Sep 1;36(9):1176-81. doi: 10.1016/j.clinthera.2014.08.010. Clin Ther. 2014. PMID: 25234549 Review.
-
[Preventing cerebrovascular accidents during atrial fibrillation].Presse Med. 2005 Oct 22;34(18):1315-24. doi: 10.1016/s0755-4982(05)84180-6. Presse Med. 2005. PMID: 16269996 Review. French.
Cited by
-
Acute unilateral renal embolism: a therapeutic challenge.Thromb J. 2025 Jun 20;23(1):67. doi: 10.1186/s12959-025-00757-1. Thromb J. 2025. PMID: 40542342 Free PMC article.
-
Renal Artery Thrombosis Leading to Renal Infarct in a Patient With Recurrent Nephrolithiasis.Cureus. 2023 Apr 26;15(4):e38169. doi: 10.7759/cureus.38169. eCollection 2023 Apr. Cureus. 2023. PMID: 37252572 Free PMC article.
-
Machine learning for risk prediction of acute kidney injury in patients with diabetes mellitus combined with heart failure during hospitalization.Sci Rep. 2025 Mar 28;15(1):10728. doi: 10.1038/s41598-025-87268-1. Sci Rep. 2025. PMID: 40155666 Free PMC article.
References
-
- Yousif A, Samannan R, Abu-Fadel M. Unilateral acute renal artery embolism: an index case of successful mechanical aspiration thrombectomy with use of penumbra indigo aspiration system and a review of the literature. Vasc Endovascular Surg. 2018;52(5):391–394. doi: 10.1177/1538574418764052. - DOI - PubMed
