

Cement Augmentation of Two-Level Lumbar Corpectomy Cage After Malposition: A Novel Salvage Procedure Technical Note
- PMID: 36258926
- PMCID: PMC9558766
- DOI: 10.7759/cureus.29074
Cement Augmentation of Two-Level Lumbar Corpectomy Cage After Malposition: A Novel Salvage Procedure Technical Note
Abstract
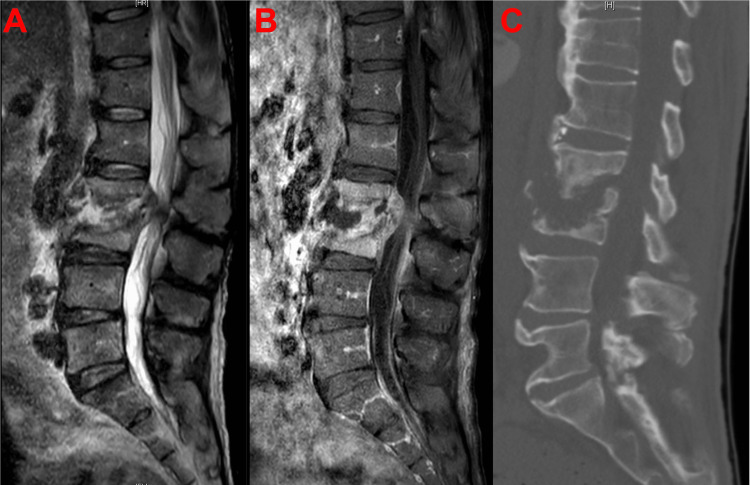
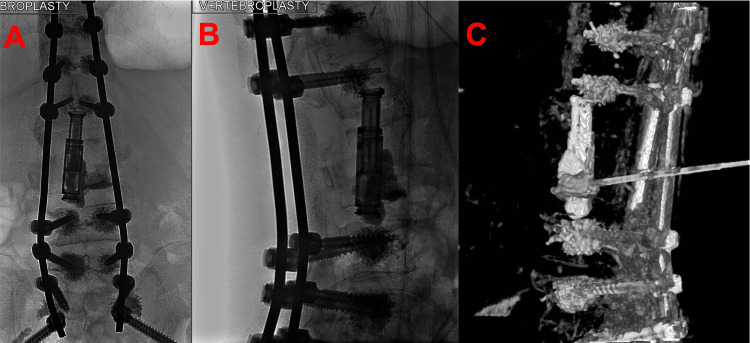
Intervertebral cage mispositioning is an uncommon complication of a posterior lumbar corpectomy. Most frequently, cages are placed obliquely, laterally, or protruding. However, there are few reports of implanted cages that fail to contact the adjacent vertebral endplate and thus no descriptions of successful revisions. The objective of this case report is to report a unique case of minimally invasive rescue vertebroplasty with cement augmentation following a lumbar corpectomy that resulted in graft-endplate noncontact in a medically complicated patient A 60-year-old male with a history of active intravenous (IV) drug use, untreated hepatitis C virus (HCV) infection, and chronic malnourishment presented with low back pain. He had a history of vertebral osteomyelitis managed with intravenous antibiotics, although he was noncompliant with infusions. The diagnosis of L2-L3 discitis-osteomyelitis with intradiscal abscess causing cord compression was made using inpatient lumbar imaging. The initial intervention was accomplished with L2 and L3 vertebral corpectomy with decompression and expandable cage placement as well as a T10-pelvis posterior fixation. Despite the resolution of presenting symptoms, routine postoperative radiographs identified noncontact between the inferior surface of the cage and the superior endplate of the L4 vertebral body. Salvage therapy was pursued via fluoroscopy-guided vertebroplasty with cement augmentation to correct cage malposition. Secondary surgical intervention was successful in bringing the intervertebral cage into contact with the adjacent vertebral body. Lower extremity strength improved, and back pain was resolved. The postoperative motor examination remained unchanged after the rescue procedure. Accurate intraoperative cage placement can be difficult in patients with poor bone quality, especially in the setting of ongoing infection and cachexia. For this reason, routine postoperative imaging is crucial to assessing graft complications. In patients who are poor candidates for revision surgery, we demonstrate that an interventional radiology-based approach may be successful in correcting cage mispositioning and preventing further changes during healing and fusion.
Keywords: cement augmentation; corpectomy; intervertebral cage; lumbar spine; neurointerventional radiology; salvage; salvage procedure; vertebral osteomyelitis; vertebroplasty.
Copyright © 2022, Hamad et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Thoracoscopic vertebral body replacement with an expandable cage after ventral spinal canal decompression. Ragel BT, Amini A, Schmidt MH. Neurosurgery. 2007;61:317–322. - PubMed
-
- Defining the indications, types and biomaterials of corpectomy cages in the thoracolumbar spine. Papanastassiou ID, Gerochristou M, Aghayev K, Vrionis FD. Expert Rev Med Devices. 2013;10:269–279. - PubMed
-
- [PEEK cage fusion after anterior cervical corpectomy : clinical and radiological results in patients with spondylotic myelopathy] Schulz C, Mauer UM, Mathieu R. Orthopade. 2017;46:242–248. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials