

Clinical Efficacy of Multidomain Interventions among Multimorbid Older People Stratified by the Status of Physio-Cognitive Declines: A Secondary Analysis from the Randomized Controlled Trial for Healthy Aging
- PMID: 36259579
- PMCID: PMC12275622
- DOI: 10.1007/s12603-022-1843-3
Clinical Efficacy of Multidomain Interventions among Multimorbid Older People Stratified by the Status of Physio-Cognitive Declines: A Secondary Analysis from the Randomized Controlled Trial for Healthy Aging
Abstract
Objectives: To investigate the clinical efficacy of integrated multidomain intervention among community-living older adults with multimorbidity and physio-cognitive decline syndrome (PCDS).
Design, setting and participants: This is the secondary analysis from a randomized controlled trial that data of 340 participants with Montreal Cognitive Assessment (MoCA) scores≥18 were excerpted for analysis.
Intervention: Sixteen 2-hour sessions per year were provided for participants, including physical exercise, cognitive training, dietician education and individualized integrated care for multimorbidity.
Measurements: Handgrip strength, 6-m walking speed, MoCA (total score and sub-domains), Cardiovascular Health Study (CHS) frailty score, quality of life, and serum biochemistry biomarkers.
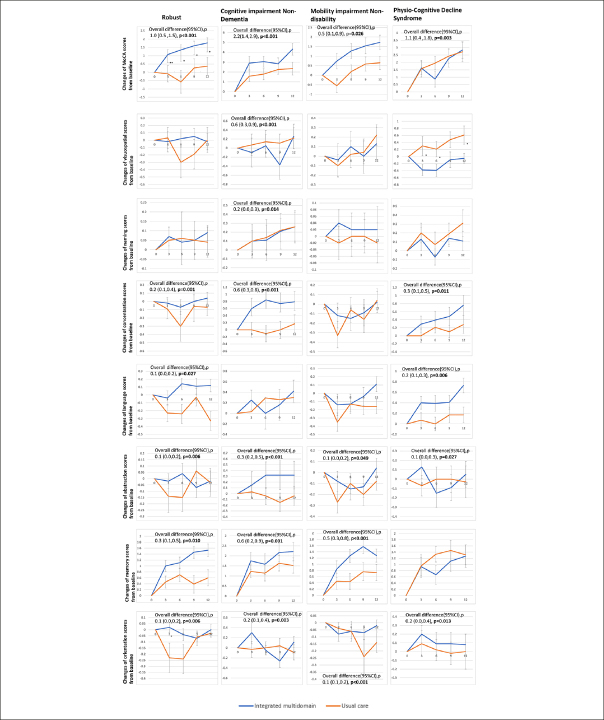
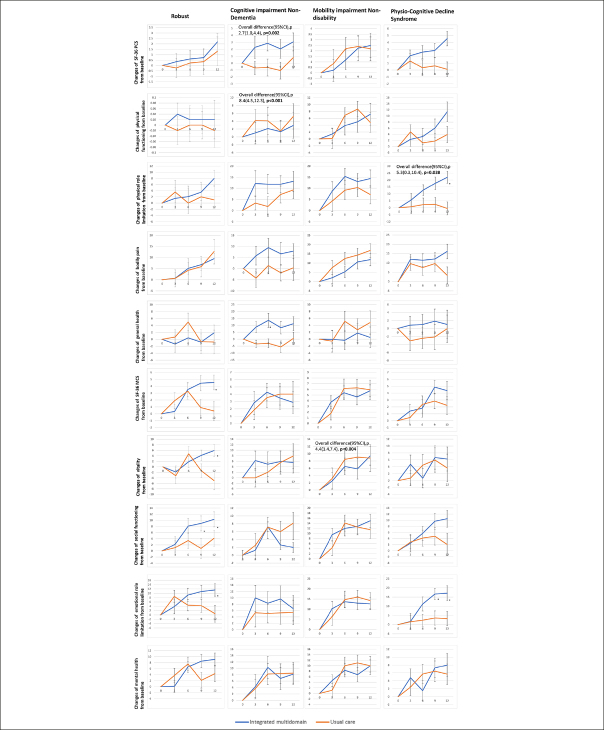
Results: Overall, 96/340 (28.2%) of all participants have PCDS, and the integrated multidomain intervention significantly improved global cognitive performance (overall difference 1.1, 95% CI 0.4 - 1.8, p=0.003), and domains of concentration (overall difference 0.3, 95%CI 0.1 - 0.5, p=0.011), language (overall difference 0.2, 95%CI 0.1 - 0.3, p=0.006), abstract thinking (overall difference 0.1, 95%CI 0.0 - 0.3, p=0.027), and orientation(overall difference 0.2, 95%CI 0.0 - 0.4, p=0.013) across all timepoints among those with PCDS. Besides, interventions also significantly reduced frailty score among those with cognitive impairment no dementia (overall difference -0.3, 95%CI -0.5 - -0.1, p=0.011) and mobility impairment no disability (overall difference -0.3, 95%CI -0.4 - -0.1, p=0.004). and improved quality of life at domain of physical role limitation among those with PCDS (overall difference 5.3, 95%CI 0.3 - 10.4, p=0.038).
Conclusions: The integrated multidomain lifestyle intervention plus multimorbidity management significantly improved cognitive function, and enhanced quality of life among older adults with multimorbidity and PCDS in the communities.
Keywords: Integrated care; cognition; frailty; multidomain intervention; physio-cognitive decline syndrome.
Conflict of interest statement
No potential conflict of interest was reported by the authors
Figures


References
-
- Beard JR, Officer A, de Carvalho IA, Sadana R, Pot AM, Michel JP, et al. The World report on ageing and health: a policy framework for healthy ageing. Lancet. 2016;387:2145–2154. 10.1016/S0140-6736(15)00516-4 PubMed PMID: 26520231. - DOI - PMC - PubMed
-
- Dixon A. The United Nations decade of healthy ageing requires concerted global action. Nature aging. 2021;1:2. 10.1038/s43587-020-00011-5 - DOI - PubMed
-
- WHO. Integrated care for older people (ICOPE): guidance for person-centred assessment and pathways in primary care. World Health Organization, 2019.
-
- Chen LK, Arai H. Physio-cognitive decline as the accelerated aging phenotype. Arch Gerontol Geriatr. 2020;88:104051. 10.1016/j.archger.2020.104051 PubMed PMID: 32278485. - DOI - PubMed
Uncited references
-
- White J, Sofat R, Hemani G, Shah T, Engmann J, Dale C, et al. Plasma urate concentration and risk of coronary heart disease: a Mendelian randomisation analysis. Lancet Diabetes Endocrinol. 2016;4:327–336. 10.1016/S2213-8587(15)00386-1 PubMed PMCID: 4805857. PubMed PMID: 26781229. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
