

Intraventricular B7-H3 CAR T Cells for Diffuse Intrinsic Pontine Glioma: Preliminary First-in-Human Bioactivity and Safety
- PMID: 36259971
- PMCID: PMC9827115
- DOI: 10.1158/2159-8290.CD-22-0750
Intraventricular B7-H3 CAR T Cells for Diffuse Intrinsic Pontine Glioma: Preliminary First-in-Human Bioactivity and Safety
Abstract
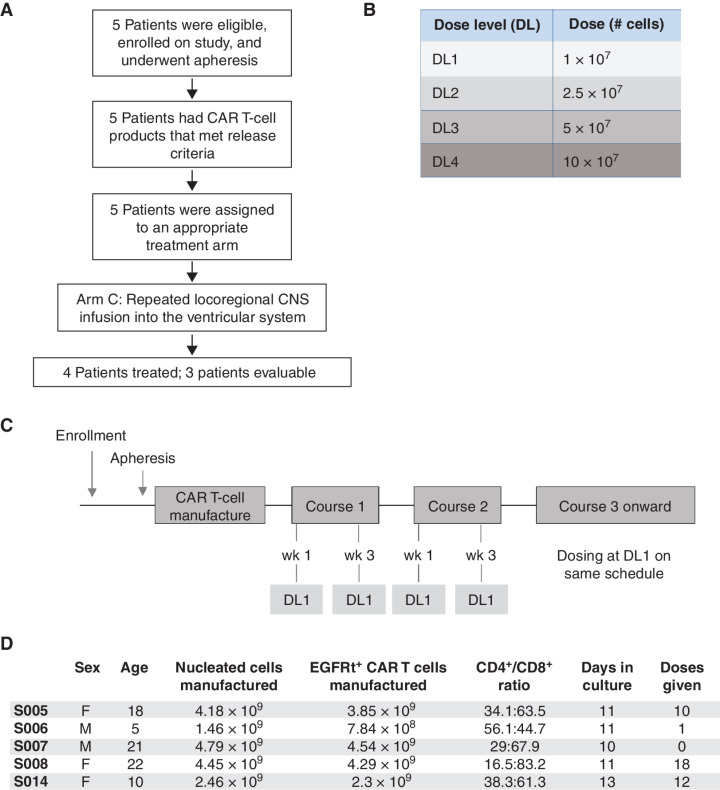
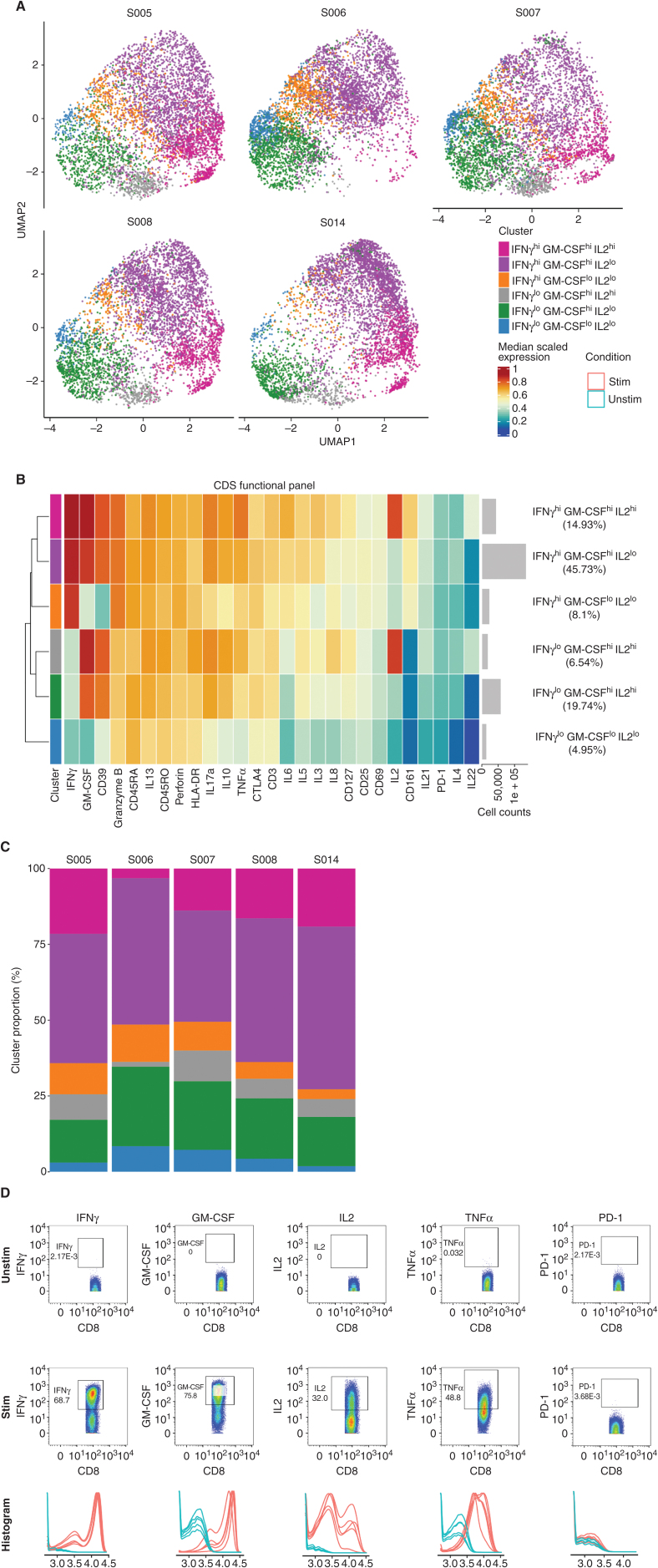
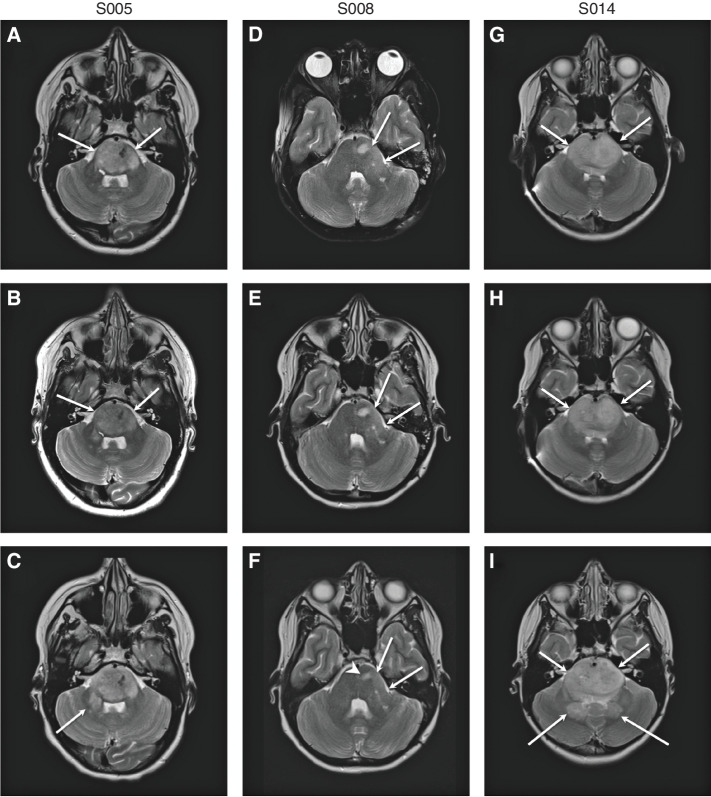
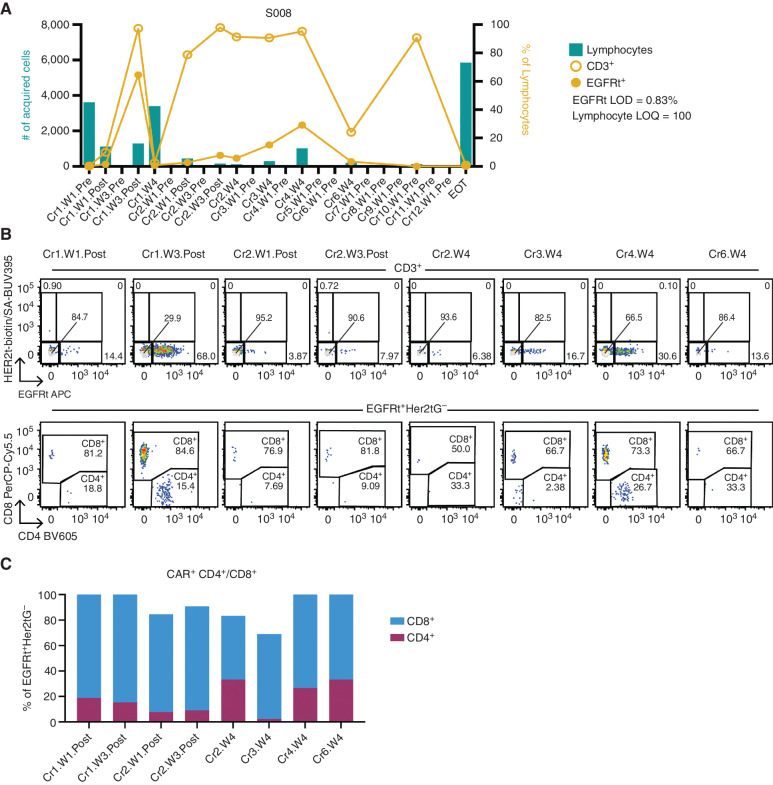
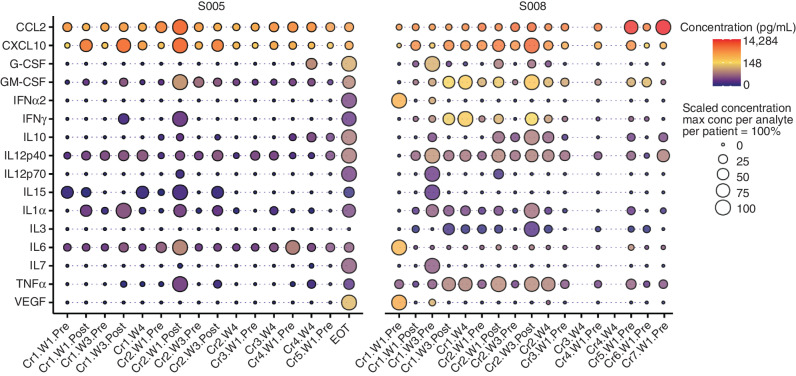
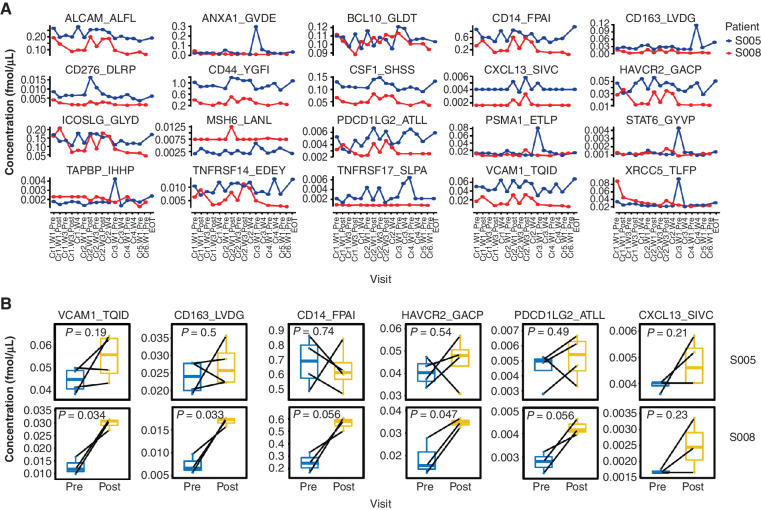
Diffuse intrinsic pontine glioma (DIPG) remains a fatal brainstem tumor demanding innovative therapies. As B7-H3 (CD276) is expressed on central nervous system (CNS) tumors, we designed B7-H3-specific chimeric antigen receptor (CAR) T cells, confirmed their preclinical efficacy, and opened BrainChild-03 (NCT04185038), a first-in-human phase I trial administering repeated locoregional B7-H3 CAR T cells to children with recurrent/refractory CNS tumors and DIPG. Here, we report the results of the first three evaluable patients with DIPG (including two who enrolled after progression), who received 40 infusions with no dose-limiting toxicities. One patient had sustained clinical and radiographic improvement through 12 months on study. Patients exhibited correlative evidence of local immune activation and persistent cerebrospinal fluid (CSF) B7-H3 CAR T cells. Targeted mass spectrometry of CSF biospecimens revealed modulation of B7-H3 and critical immune analytes (CD14, CD163, CSF-1, CXCL13, and VCAM-1). Our data suggest the feasibility of repeated intracranial B7-H3 CAR T-cell dosing and that intracranial delivery may induce local immune activation.
Significance: This is the first report of repeatedly dosed intracranial B7-H3 CAR T cells for patients with DIPG and includes preliminary tolerability, the detection of CAR T cells in the CSF, CSF cytokine elevations supporting locoregional immune activation, and the feasibility of serial mass spectrometry from both serum and CSF. This article is highlighted in the In This Issue feature, p. 1.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures
Comment in
References
-
- Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, et al. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol 2016;131:803–20. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
