

Management of chyluria using percutaneous thoracic duct stenting
- PMID: 36260143
- PMCID: PMC9582170
- DOI: 10.1186/s42155-022-00333-y
Management of chyluria using percutaneous thoracic duct stenting
Abstract
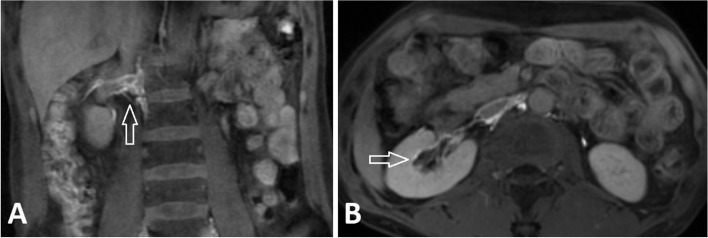
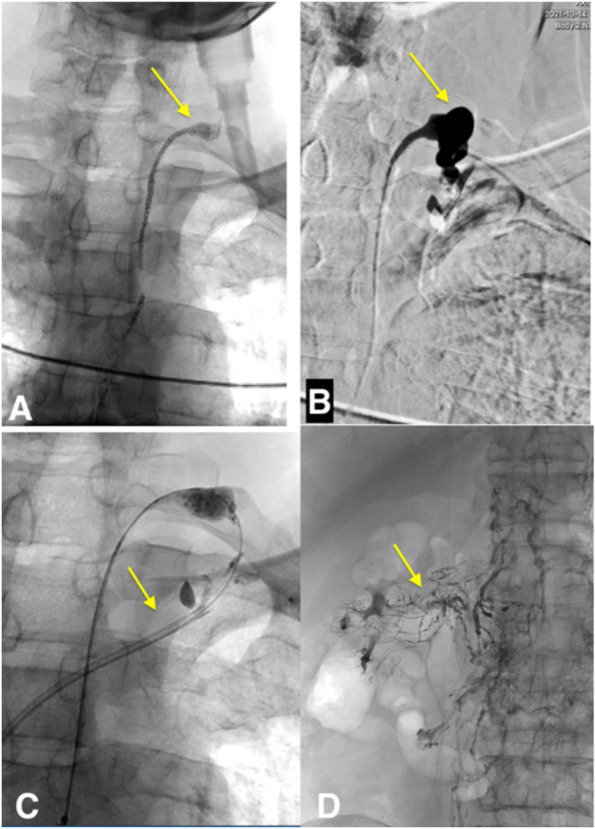
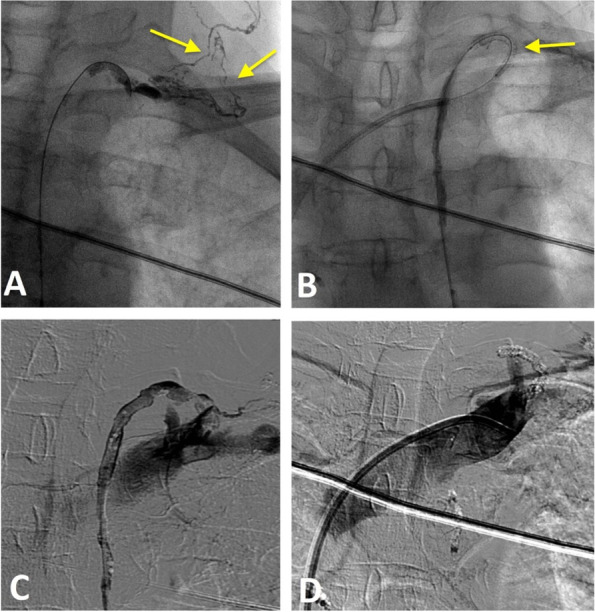
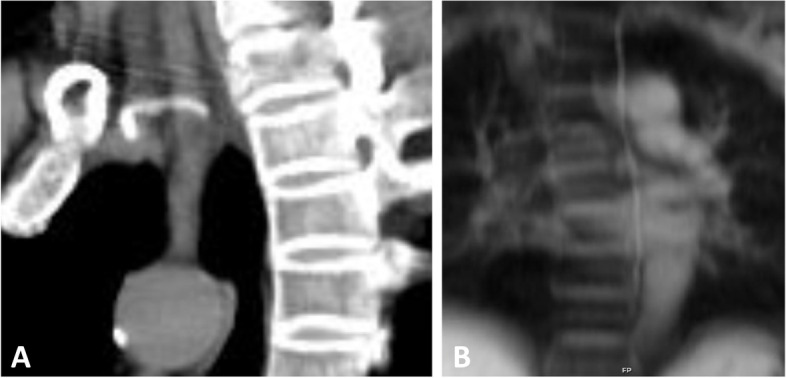
Background: Thoracic duct stenosis or obstruction is one of the causes of chyluria. Although the diagnosis of chyluria is not difficult, treatment is still challenging. Although there have been no standard guidelines for the treatment of chyluria, interventional techniques now offer minimally invasive treatment options for chyluria such as interstitial lymphatic embolization, ductoplasty with balloon, or thoracic duct stenting. CASE PRESENTATION : Here, we report a case of chyluria due to obstruction of the junction between the thoracic duct and subclavian vein in a 64 -year- old female patient. The patient was treated with balloon plasty for lymphovenous junction obstruction and interstitial lymphatic embolization for chyluria. However, chyluria was recurrent after 6 months so intranodal lymphangiography was performed. Anterograde thoracic duct was accessed through a transabdominal to the cisterna chyli which showed that the thoracic venous junction was re-obstruction. The patient was successfully treated by placing a uncovered drug-eluting stent with the size of 2.5 mm x 15 mm in length for resolving the thoracic occlusion.
Conclusion: This report demonstrates the feasibility of using thoracic duct stenting in the treatment chyluria due to lymphovenous junction obstruction.
Keywords: Balloon; Chyluria; Lymphatic; Obstruction; Stenosis; Stent; Thoracic duct.
© 2022. The Author(s).
Conflict of interest statement
All authors declare that they have no conflict of interest.
Figures
References
-
- Chick JFB, Hage AN, Patel N, Gemmete JJ, Meadows JM, Srinivasa RN. Chylothorax secondary to venous outflow obstruction treated with transcervical retrograde thoracic duct cannulation with embolization and venous reconstruction. J Vascular Surg Cases Innovations Techniques. 2018;4(3):193–196. doi: 10.1016/j.jvscit.2018.03.010. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources