

Current state of high-fidelity multimodal monitoring in traumatic brain injury
- PMID: 36260235
- PMCID: PMC9705453
- DOI: 10.1007/s00701-022-05383-8
Current state of high-fidelity multimodal monitoring in traumatic brain injury
Abstract
Introduction: Multimodality monitoring of patients with severe traumatic brain injury (TBI) is primarily performed in neuro-critical care units to prevent secondary harmful brain insults and facilitate patient recovery. Several metrics are commonly monitored using both invasive and non-invasive techniques. The latest Brain Trauma Foundation guidelines from 2016 provide recommendations and thresholds for some of these. Still, high-level evidence for several metrics and thresholds is lacking.
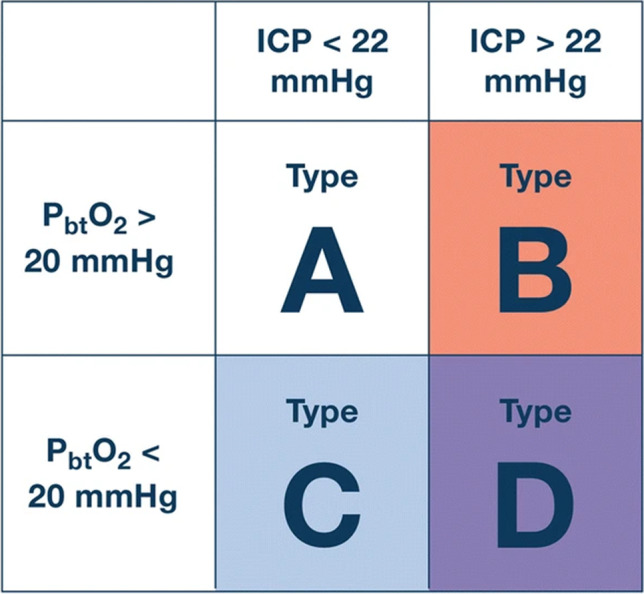
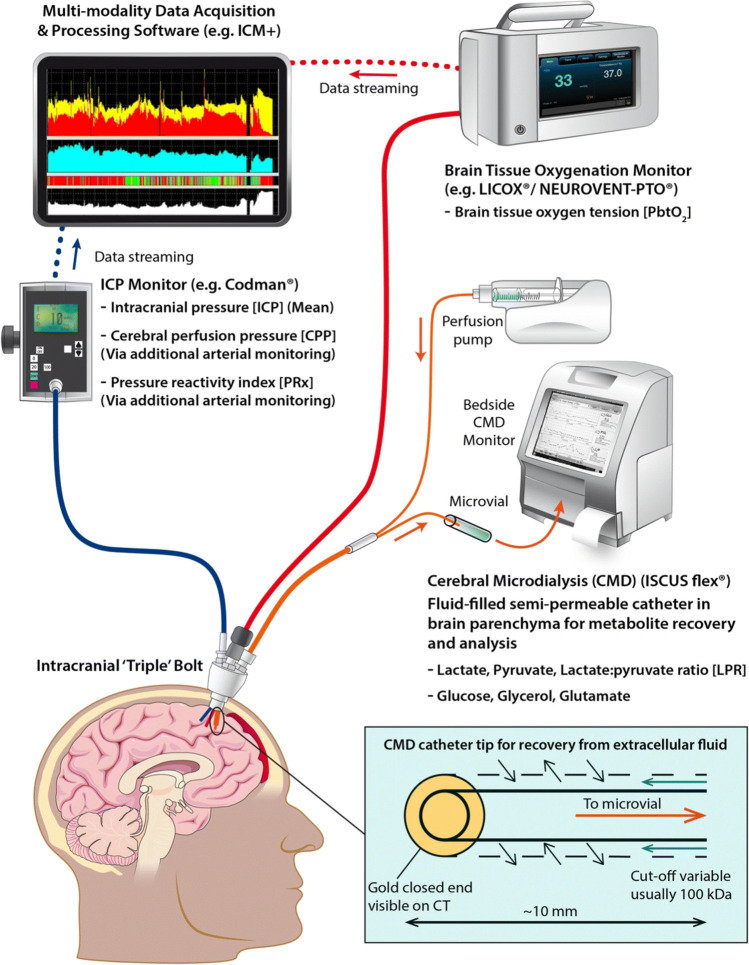
Methods: Regarding invasive brain monitoring, intracranial pressure (ICP) forms the cornerstone, and pressures above 22 mmHg should be avoided. From ICP, cerebral perfusion pressure (CPP) (mean arterial pressure (MAP)-ICP) and pressure reactivity index (PRx) (a correlation between slow waves MAP and ICP as a surrogate for cerebrovascular reactivity) may be derived. In terms of regional monitoring, partial brain tissue oxygen pressure (PbtO2) is commonly used, and phase 3 studies are currently ongoing to determine its added effect to outcome together with ICP monitoring. Cerebral microdialysis (CMD) is another regional invasive modality to measure substances in the brain extracellular fluid. International consortiums have suggested thresholds and management strategies, in spite of lacking high-level evidence. Although invasive monitoring is generally safe, iatrogenic hemorrhages are reported in about 10% of cases, but these probably do not significantly affect long-term outcome. Non-invasive monitoring is relatively recent in the field of TBI care, and research is usually from single-center retrospective experiences. Near-infrared spectrometry (NIRS) measuring regional tissue saturation has been shown to be associated with outcome. Transcranial doppler (TCD) has several tentative utilities in TBI like measuring ICP and detecting vasospasm. Furthermore, serial sampling of biomarkers of brain injury in the blood can be used to detect secondary brain injury development.
Conclusions: In multimodal monitoring, the most important aspect is data interpretation, which requires knowledge of each metric's strengths and limitations. Combinations of several modalities might make it possible to discern specific pathologic states suitable for treatment. However, the cost-benefit should be considered as the incremental benefit of adding several metrics has a low level of evidence, thus warranting additional research.
Keywords: Biomarkers; Intracranial pressure; Multimodal monitoring; Neuro-critical care; Traumatic brain injury.
© 2022. The Author(s).
Figures
References
-
- Akerlund CA, Donnelly J, Zeiler FA, Helbok R, Holst A, Cabeleira M, Guiza F, Meyfroidt G, Czosnyka M, Smielewski P, Stocchetti N, Ercole A, Nelson DW, Participants C-THRIS-S, Investigators Impact of duration and magnitude of raised intracranial pressure on outcome after severe traumatic brain injury: a CENTER-TBI high-resolution group study. PLoS One. 2020;15:e0243427. doi: 10.1371/journal.pone.0243427. - DOI - PMC - PubMed
-
- Aries MJ, Czosnyka M, Budohoski KP, Steiner LA, Lavinio A, Kolias AG, Hutchinson PJ, Brady KM, Menon DK, Pickard JD, Smielewski P. Continuous determination of optimal cerebral perfusion pressure in traumatic brain injury. Crit Care Med. 2012;40:2456–2463. doi: 10.1097/CCM.0b013e3182514eb6. - DOI - PubMed
-
- Bernard F, Barsan W, Diaz-Arrastia R, Merck LH, Yeatts S, Shutter LA. Brain Oxygen Optimization in Severe Traumatic Brain Injury (BOOST-3): a multicentre, randomised, blinded-endpoint, comparative effectiveness study of brain tissue oxygen and intracranial pressure monitoring versus intracranial pressure alone. BMJ Open. 2022;12:e060188. doi: 10.1136/bmjopen-2021-060188. - DOI - PMC - PubMed
-
- Birg T, Ortolano F, Wiegers EJA, Smielewski P, Savchenko Y, Ianosi BA, Helbok R, Rossi S, Carbonara M, Zoerle T, Stocchetti N, Investigators C-T, Participants, Brain temperature influences intracranial pressure and cerebral perfusion pressure after traumatic brain injury: a CENTER-TBI study. Neurocrit Care. 2021;35:651–661. doi: 10.1007/s12028-021-01294-1. - DOI - PMC - PubMed
-
- Carney N, Totten AM, O’Reilly C, Ullman JS, Hawryluk GW, Bell MJ, Bratton SL, Chesnut R, Harris OA, Kissoon N, Rubiano AM, Shutter L, Tasker RC, Vavilala MS, Wilberger J, Wright DW, Ghajar J. Guidelines for the management of severe traumatic brain injury, Fourth Edition. Neurosurgery. 2017;80:6–15. doi: 10.1227/NEU.0000000000001432. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
