

Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease Presenting as Intracranial Hypertension: A Case Report
- PMID: 36261298
- PMCID: PMC9581460
- DOI: 10.1212/NXI.0000000000200020
Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease Presenting as Intracranial Hypertension: A Case Report
Abstract
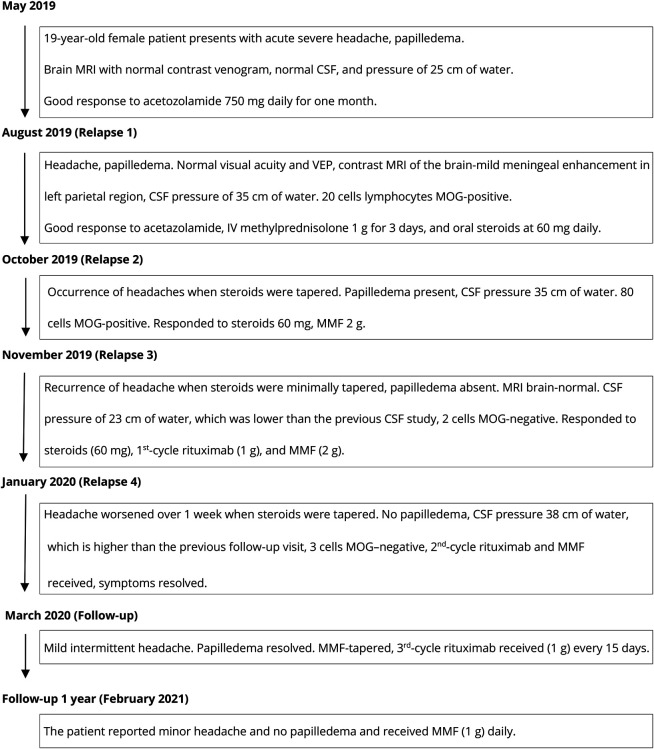
The production of autoantibodies against myelin oligodendrocyte glycoprotein (MOG) can cause a spectrum of autoimmune disorders, including optic neuritis, transverse myelitis, brainstem encephalitis, and acute disseminated encephalomyelitis. In this study, we present the case of a 19-year-old woman with an unusual clinical presentation of intracranial hypertension (IH) and bilateral papilledema. The patient presented with symptoms of increased intracranial pressure, which followed a relapsing, remitting course over several months. Serial CSF studies showed an increased opening pressure during clinical relapses. The CSF and serum tested positive for MOG immunoglobulin G antibodies. Contrast-enhanced MRI of the brain showed mild meningeal enhancement in the left parietal region with subtle underlying cortical hyperintensities, indicating possible fluid-attenuated inversion recovery variable unilateral enhancement of the leptomeninges. The patient responded well to immunosuppressive therapy using rituximab. The presentation of MOG antibody-associated disease (MOGAD) as IH without optic neuritis is rare. This report presents the first description of a relapsing remitting course presenting each time with only symptoms of raised intracranial pressure, without developing any typical clinical manifestations of MOGAD.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures

References
-
- Netravati M, Holla VV, Nalini A, et al. . Myelin oligodendrocyte glycoprotein-antibody-associated disorder: a new inflammatory CNS demyelinating disorder. J Neurol. 2021;268(4):1419-1433. - PubMed
-
- Hacohen Y, Rossor T, Mankad K, et al. . ‘Leukodystrophy-like’ phenotype in children with myelin oligodendrocyte glycoprotein antibody-associated disease. Dev Med Child Neurol. 2018;60(4):417-423. - PubMed
-
- Corbett J, Bhuta S, Prain K, Brilot F, Sabet A, Broadley SA. PRES-like presentation in MOG antibody-related demyelination (MARD). J Clin Neurosci. 2020;72:453-455. - PubMed
-
- Narayan RN, Wang C, Sguigna P, Husari K, Greenberg B. Atypical Anti-MOG syndrome with aseptic meningoencephalitis and pseudotumor cerebri-like presentations. Mult Scler Relat Disord. 2019;27:30-33. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources