

Systematic review and meta-analysis of head-to-head trials comparing sulfonylureas and low hypoglycaemic risk antidiabetic drugs
- PMID: 36261824
- PMCID: PMC9580135
- DOI: 10.1186/s12902-022-01158-5
Systematic review and meta-analysis of head-to-head trials comparing sulfonylureas and low hypoglycaemic risk antidiabetic drugs
Abstract
Background: Safety of sulfonylurea drugs in the treatment of Type 2 Diabetes is still under debate. The aim of this study was to compare the all-cause mortality and cardiovascular adverse events of sulfonylureas and drugs with a low risk for hypoglycaemia in adults with type 2 diabetes.
Methods: Systematic review and meta-analysis of randomised controlled trials.
Data sources: MEDLINE (PubMed, OVID), Embase, Cochrane Central Register of Controlled Trials, CINAHL, WOS and Lilacs.
Study selection: Randomised controlled head-to-head trials that compared sulfonylureas with active control with low hypoglycaemic potential in adults (≥ 18 years old) with type 2 diabetes published up to August 2015. The drug classes involved in the analysis were metformin, dipeptidyl peptidase-4 (DPP-4) inhibitors, sodium-glucose co-transporter-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists.
Outcomes: The primary endpoint was all-cause mortality. The secondary endpoints were MACE, cardiovascular events and severe hypoglycaemia.
Synthesis of results: Two reviewers checked study eligibility, independently extracted data and assessed quality with disagreements resolved through discussion. We assessed the risk of bias of the included studies using the Cochrane risk of bias tool for randomized trials v2. Pooled odds ratios (ORs) were estimated by using fixed effects model. The study is registered on PROSPERO (26/05/2016 CRD42016038780).
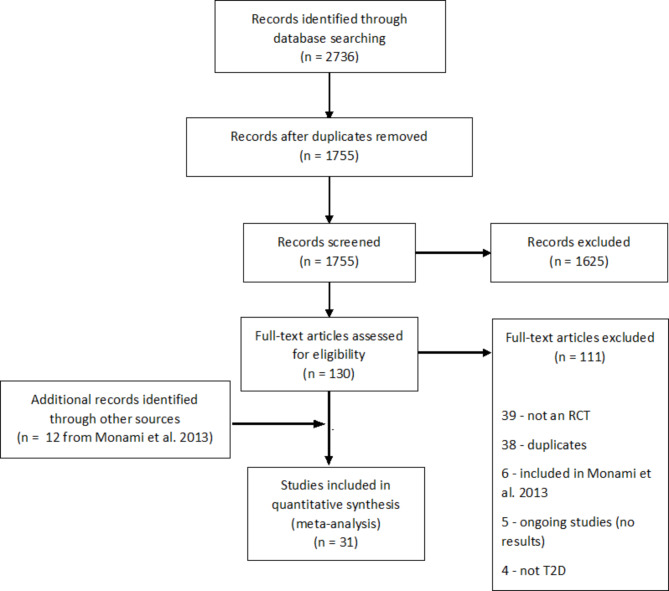
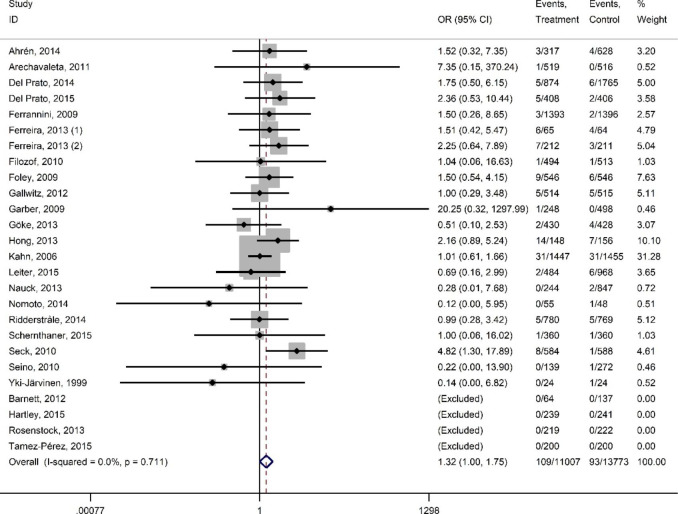
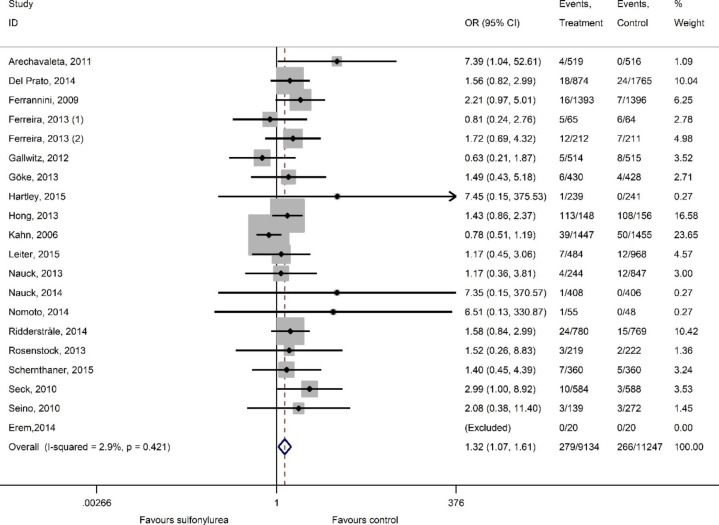
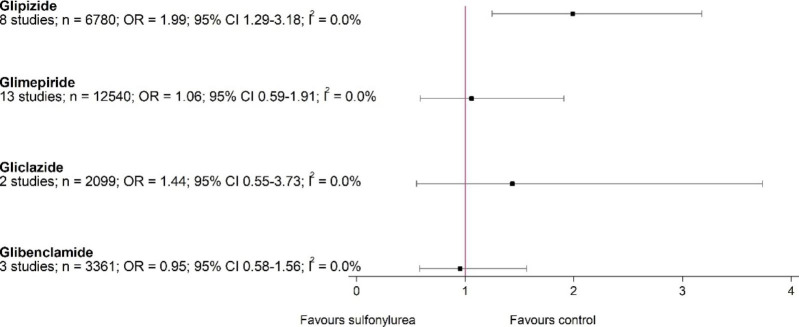
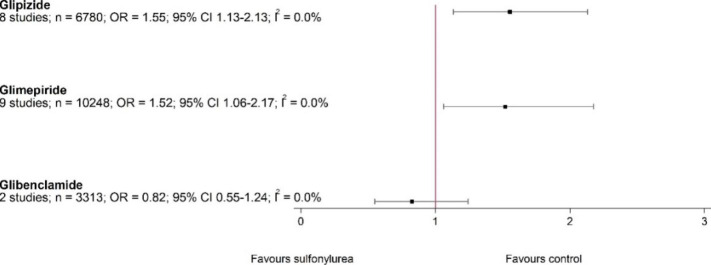
Results: Our final analysis comprised 31 studies (26,204 patients, 11,711 patients given sulfonylureas and 14,493 given comparator drugs). In comparison to drugs with low hypoglycaemic potential, sulfonylureas had higher odds for all-cause mortality (OR 1.32, 95% CI 1.00-1.75), MACE (OR 1.32, 95% CI 1.07-1.61), myocardial infarction (fatal and non-fatal) (OR 1.67, 95% CI 1.17-2.38) and hypoglycaemia (OR 5.24, 95% CI 4.20-6.55). Subsequent sensitivity analysis revealed differences in the effect of sulfonylureas, with an increased risk of all-cause mortality with glipizide but not the other molecules.
Conclusion: Our meta-analysis raises concern about the safety of SUs compared to alternative drugs involved in current analysis. Important differences may exist within the drug class, and glimepiride seems to have best safety profile.
Keywords: All-cause mortality; Diabetes mellitus; Hypoglycemic therapy; MACE; Sulfonylurea.
© 2022. The Author(s).
Conflict of interest statement
Vallo Volke has served at speakers’ bureau and received travel grants from Novo Nordisk; Eli Lilly; Aventis, Astra Zeneca and Boehringer Ingelheim. The remaining authors have declared that no conflict of interest exists.
Figures

References
-
- Ambos A, Raie E, Kiudma T, et al. 2. Tüüpi diabeedi Eesti ravijuhend 2016. Eesti Arst. 2016;95:465–73. doi: 10.15157/ea.v0i0.13016. - DOI
-
- Buse JB, Wexler DJ, Tsapas A, et al. 2019 Update to: Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) Diabetes Care. 2020;43:487–93. doi: 10.2337/DCI19-0066. - DOI - PMC - PubMed
-
- Meinert CL, Knatterud GL, Prout TE, et al. A study of the effects of hypoglycemic agents on vascular complications in patients with adult-onset diabetes. II. Mortality results. Diabetes. 1970;19:uppl–830. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
