

Association of stress hyperglycemia ratio and in-hospital mortality in patients with coronary artery disease: insights from a large cohort study
- PMID: 36261839
- PMCID: PMC9580448
- DOI: 10.1186/s12933-022-01645-y
Association of stress hyperglycemia ratio and in-hospital mortality in patients with coronary artery disease: insights from a large cohort study
Abstract
Background: Stress hyperglycemia is strongly associated with poor clinical outcomes in patients with acute coronary syndrome (ACS). Recently, the stress hyperglycemia ratio (SHR) has been proposed to represent relative hyperglycemia. Studies regarding the relationship between SHR and mortality in coronary artery disease (CAD) are limited. This study aimed to clarify the association between SHR and in-hospital mortality in patients with CAD.
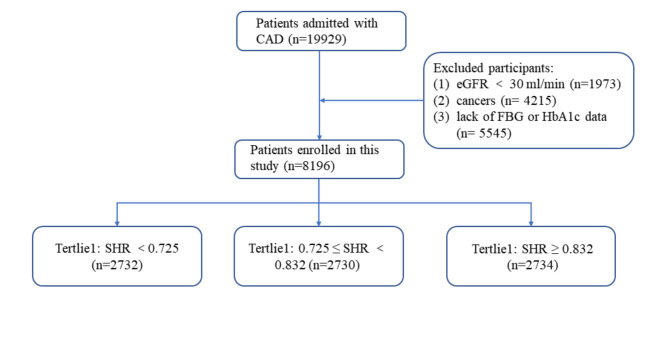
Methods: A total of 19,929 patients with CAD who were hospitalized in Beijing Hospital were enrolled in this study. Patients with an estimated glomerular filtration rate < 30 ml/min, cancer, or missing blood glucose/HbA1c data were excluded; therefore, 8,196 patients were included in the final analysis. The patients were divided into three groups based on tertiles of SHR: T1 group (SHR < 0.725, n = 2,732), T2 group (0.725 ≤ SHR < 0.832, n = 2,730), and T3 group (SHR ≥ 0.832, n = 2,734). The primary endpoint was in-hospital mortality.
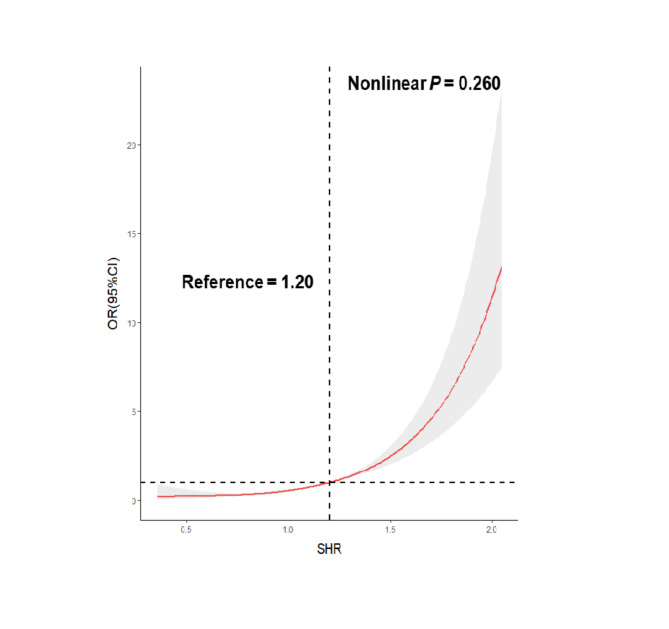
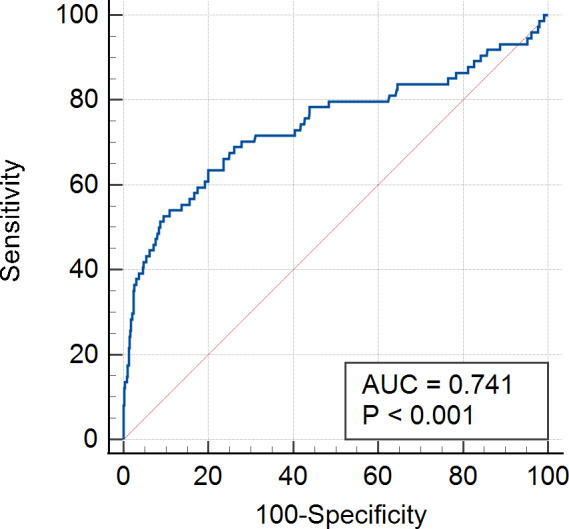
Results: The overall in-hospital mortality rate was 0.91% (n = 74). After adjusting for covariates, SHR was significantly associated with in-hospital mortality in patients with CAD [odds ratio (OR) = 17.038; 95% confidence interval (CI) = 9.668-30.027; P < 0.001], and the T3 group had a higher risk of in-hospital mortality (OR = 4.901; 95% CI = 2.583-9.297; P < 0.001) compared with T1 group. In the subgroup analysis, the T3 group had an increased risk of mortality among patients with pre-diabetes mellitus (pre-DM) (OR = 9.670; 95% CI = 1.886-49.571; P = 0.007) and diabetes mellitus (DM) (OR = 5.023; 95% CI = 2.371-10.640; P < 0.001) after adjustments for covariates. The relationship between SHR and in-hospital mortality among patients with ACS and chronic coronary syndrome was consistent with the main finding. SHR and in-hospital mortality exhibited a dose-response relationship, and the risk of in-hospital mortality increased when the SHR index was above 1.20. Moreover, the area under the curve of SHR for predicting in-hospital mortality in patients with CAD was 0.741.
Conclusion: SHR is significantly associated with in-hospital mortality in patients with CAD. SHR may be an effective predictor of in-hospital mortality in patients with CAD, especially for those with pre-DM and DM.
Keywords: Coronary artery disease; Diabetes; Mortality; Stress hyperglycemia; Stress hyperglycemia ratio.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no conflicts of interest regarding the submitted work.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
