

Evolution of ultrasound in giant cell arteritis
- PMID: 36262280
- PMCID: PMC9574015
- DOI: 10.3389/fmed.2022.981659
Evolution of ultrasound in giant cell arteritis
Abstract
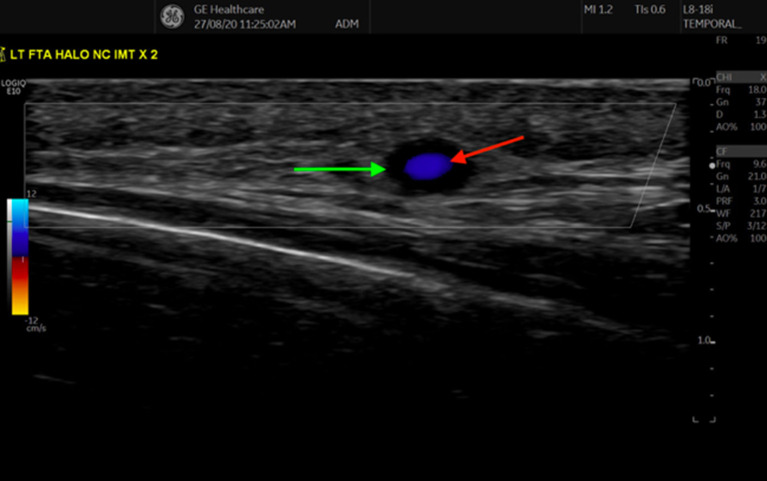
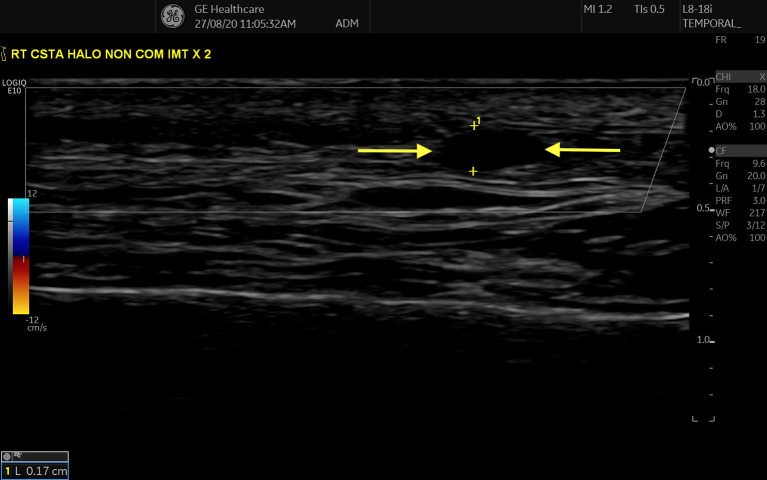
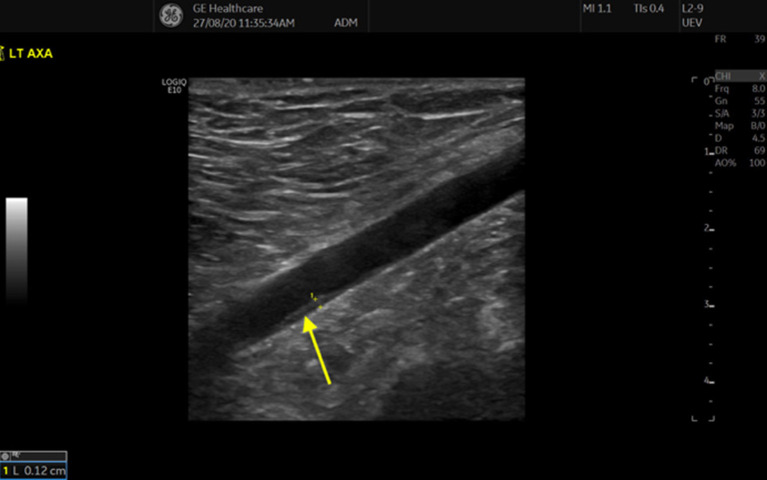
Ultrasound (US) is being increasingly used to diagnose Giant Cell Arteritis (GCA). The traditional diagnostic Gold Standard has been temporal artery biopsy (TAB), but this is expensive, invasive, has a false-negative rate as high as 60% and has little impact on clinical decision-making. A non-compressible halo with a thickened intima-media complex (IMC) is the sonographic hallmark of GCA. The superficial temporal arteries (STA) and axillary arteries (AA) are the most consistently inflamed arteries sonographically and imaging protocols for evaluating suspected GCA should include at least these two arterial territories. Studies evaluating temporal artery ultrasound (TAUS) have varied considerably in size and methodology with results showing wide discrepancies in sensitivity (9-100%), specificity (66-100%), positive predictive value (36-100%) and negative predictive value (33-100%). Bilateral halos increase sensitivity as does the incorporation of pre-test probability, while prior corticosteroid use decreases sensitivity. Quantifying sonographic vasculitis using Halo Counts and Halo Scores can predict disease extent/severity, risk of specific complications and likelihood of treatment response. Regression of the Halo sign has been observed from as little as 2 days to as late as 7 months after initiation of immunosuppressive treatment and occurs at different rates in STAs than AAs. US is more sensitive than TAB and has comparable sensitivity to MRI and PET/CT. It is time-efficient, cost-effective and allows for the implementation of fast-track GCA clinics which substantially mitigate the risk of irreversible blindness. Algorithms incorporating combinations of imaging modalities can achieve a 100% sensitivity and specificity for a diagnosis of GCA. US should be a standard first line investigation in routine clinical care of patients with suspected GCA with TAB reserved only for those having had a normal US in the context of a high pre-test probability.
Keywords: biomarkers; giant cell (temporal) arteritis; large vessel vasculitis; temporal artery biopsy; ultrasound.
Copyright © 2022 Kirby, Flood, Mullan, Murphy and Kane.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Duftner C, Dejaco C, Sepriano A, Falzon L, Schmidt WA, Ramiro S. Imaging in diagnosis, outcome prediction and monitoring of large vessel vasculitis: a systematic literature review and meta-analysis informing the EULAR recommendations. RMD open. (2018) 4:e000612. 10.1136/rmdopen-2017-000612 - DOI - PMC - PubMed
-
- Luqmani R, Lee E, Singh S, Gillett M, Schmidt WA, Bradburn M, et al. . The role of ultrasound compared to biopsy of temporal arteries in the diagnosis and treatment of giant cell arteritis (TABUL): a diagnostic accuracy and cost-effectiveness study. Health Technol Assess. (2016) 20:1–238. 10.3310/hta20900 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources