

Serological responses to human virome define clinical outcomes of Italian patients infected with SARS-CoV-2
- PMID: 36263161
- PMCID: PMC9576512
- DOI: 10.7150/ijbs.78002
Serological responses to human virome define clinical outcomes of Italian patients infected with SARS-CoV-2
Abstract
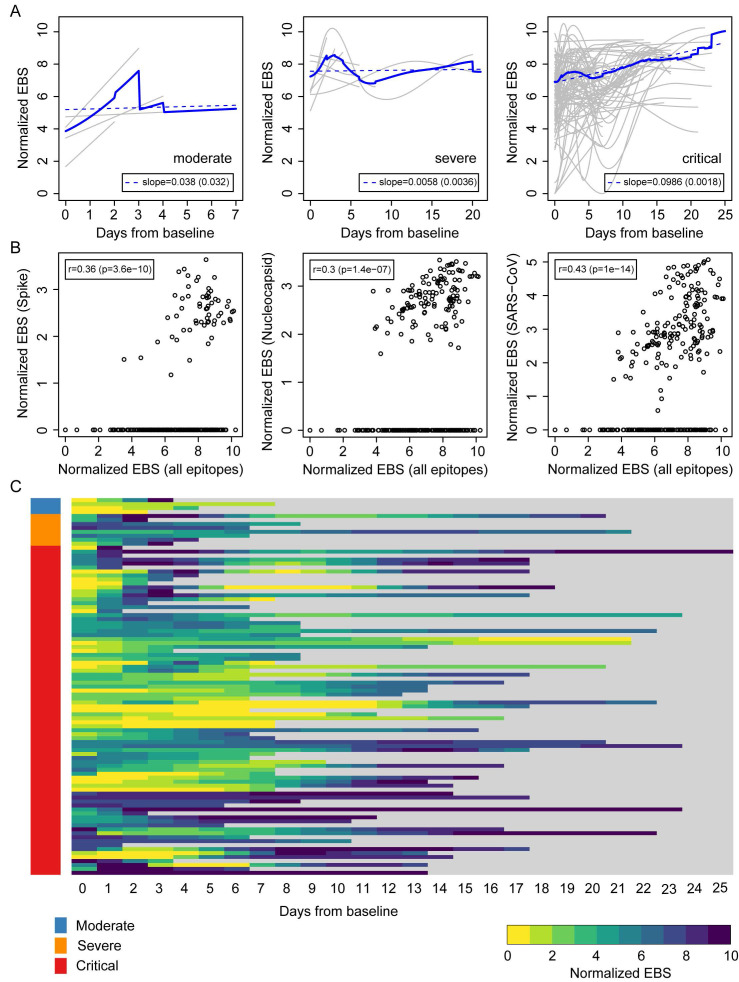
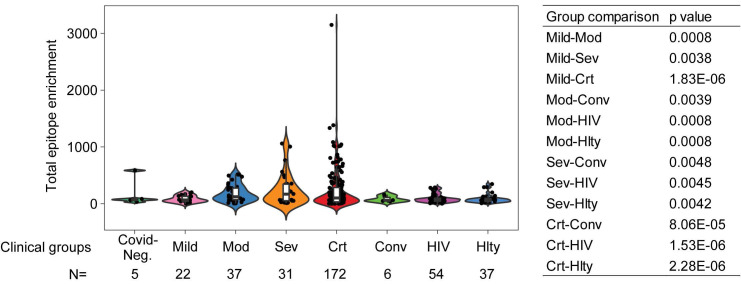
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is responsible for the pandemic respiratory infectious disease COVID-19. However, clinical manifestations and outcomes differ significantly among COVID-19 patients, ranging from asymptomatic to extremely severe, and it remains unclear what drives these disparities. Here, we studied 159 sequentially enrolled hospitalized patients with COVID-19-associated pneumonia from Brescia, Italy using the VirScan phage-display method to characterize circulating antibodies binding to 96,179 viral peptides encoded by 1,276 strains of human viruses. SARS-CoV-2 infection was associated with a marked increase in immune antibody repertoires against many known pathogenic and non-pathogenic human viruses. This antiviral antibody response was linked to longitudinal trajectories of disease severity and was further confirmed in additional 125 COVID-19 patients from the same geographical region in Northern Italy. By applying a machine-learning-based strategy, a viral exposure signature predictive of COVID-19-related disease severity linked to patient survival was developed and validated. These results provide a basis for understanding the role of memory B-cell repertoire to viral epitopes in COVID-19-related symptoms and suggest that a unique anti-viral antibody repertoire signature may be useful to define COVID-19 clinical severity.
© The author(s).
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures



Update of
-
Serological Responses to Human Virome Define Clinical Outcomes of Italian Patients Infected with SARS-CoV-2.medRxiv [Preprint]. 2020 Sep 7:2020.09.04.20187088. doi: 10.1101/2020.09.04.20187088. medRxiv. 2020. Update in: Int J Biol Sci. 2022 Sep 1;18(15):5591-5606. doi: 10.7150/ijbs.78002. PMID: 32908997 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
