

Neurophysiological differentiation of upper motor neuron damage in neurodegenerative disorders
- PMID: 36263296
- PMCID: PMC9574772
- DOI: 10.1016/j.cnp.2022.09.002
Neurophysiological differentiation of upper motor neuron damage in neurodegenerative disorders
Abstract
Objective: Using transcranial magnetic stimulation (TMS) to delineate upper motor neuron (UMN) signs of two neurodegenerative disorders: amyotrophic lateral sclerosis (ALS) and multiple system atrophy (MSA).
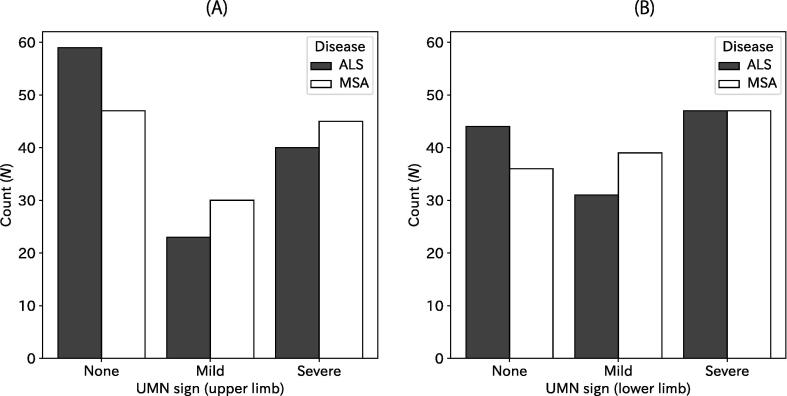
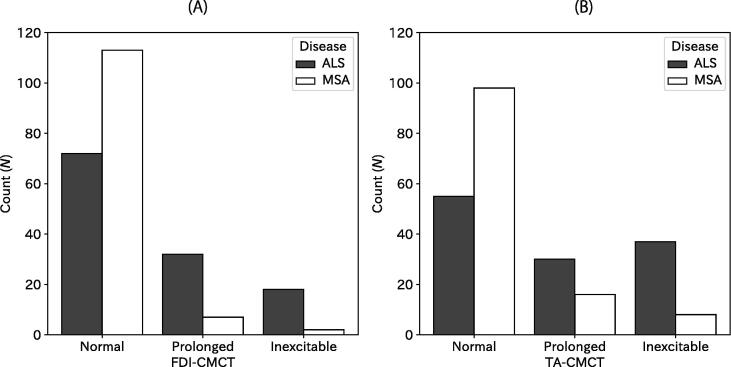
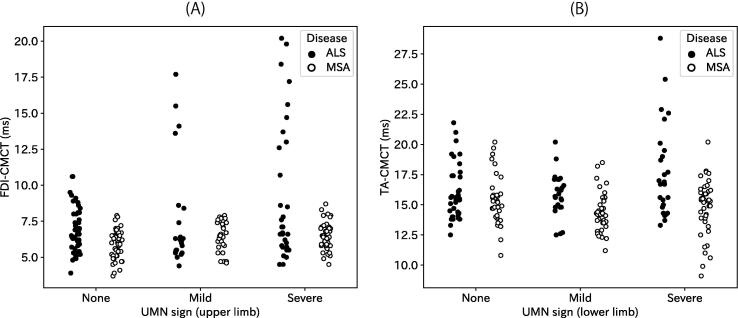
Methods: Medical records including clinical signs for UMN damage and TMS results were reviewed retrospectively. The UMN signs were classified into none, mild, and severe based on neurological examination of various reflexes. Then TMS-elicited motor evoked potentials (MEPs) were recorded from a hand and a leg muscle to calculate the central motor conduction time (CMCT), which represents fast, mono-synaptic conduction along the corticospinal tract. Relations between the UMN signs and CMCT were analysed for the two diseases.
Results: Prevalence and severity of the UMN signs for ALS and MSA were comparable for both upper and lower limbs. However, abnormality in CMCT was found more frequently in ALS: CMCT abnormalities were found in upper limbs for 44% in ALS patients but only for 7% in MSA patients; CMCT abnormalities in lower limbs were 55% in ALS and 20% in MSA. Some ALS patients showed abnormal CMCT in limbs without UMN signs, which was not true for most MSA patients.
Conclusions: The abnormalities of CMCT were different in ALS and MSA, even for those who clinically had similar UMN signs. Sometimes, CMCT can reveal UMN damage in the absence of clinical UMN signs. Differences presumably derive from selective degeneration of different fibres in the motor descending pathways. Longitudinal studies must be conducted to accumulate neuroimaging and pathological findings.
Significance: CMCT can be useful to differentiate ALS and MSA.
Keywords: AH, Abductor halluces; ALS, Amyotrophic lateral sclerosis; ANOVA, analysis of variance; APB, Abductor pollicis brevis; Amyotrophic lateral sclerosis; CMAP, compound muscle action potential; CMCT, central motor conduction time; Central motor conduction time; EMG, electromyography; FDI, first dorsal interosseous; LMN, lower motor neuron; M1, primary motor area; MEP, motor evoked potential; MSA, multiple system atrophy; Motor evoked potential; Multiple system atrophy; Neurophysiology; Pyramidal tract; TA, tibialis anterior; TMS, transcranial magnetic stimulation; UMN, upper motor neuron.
© 2022 International Federation of Clinical Neurophysiology. Published by Elsevier B.V.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Abbruzzese G., Marchese R., Trompetto C. Sensory and motor evoked potentials in multiple system atrophy: A comparative study with Parkinson's disease. Mov. Disord. 1997;12:315–321. - PubMed
-
- Abele M., Schulz J.B., Bürk K., Topka H., Dichgans J., Klockgether T. Evoked potentials in multiple systematrophy (MSA) Acta Neurol. Scand. 2000;101:111–115. - PubMed
-
- Brooks B.R., Miller R.G., Swash M., Munsat T.L. El Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph Lateral Scler Other Motor Neuron Disord. 2000;1:293–299. - PubMed
-
- Civardi C., Collini A., Mazzini L., Monaco F., Geda C. Single-pulse transcranial magnetic stimulation in amyotrophic lateral sclerosis. Muscle Nerve. 2020;61:330–337. - PubMed
-
- Claus D. Central motor conduction: Method and normal results. Muscle Nerve. 1990;13:1125–1132. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
