

Prevalence, trend, and predictor analyses of vitamin D deficiency in the US population, 2001-2018
- PMID: 36263304
- PMCID: PMC9573946
- DOI: 10.3389/fnut.2022.965376
Prevalence, trend, and predictor analyses of vitamin D deficiency in the US population, 2001-2018
Abstract
Background: The National Health and Nutrition Examination Surveys (NHANES) collect and release data to the public every 2 years. The latest NHANES study on the vitamin D status of Americans was based on data from 2001 to 2014, and the latest data (2015-2016 and 2017-2018) have not been studied yet. Thus, we extracted all the available data from NHANES (2001-2018), aiming to analyze the prevalence and trends of vitamin D deficiency (VDD) in the US population to bridge the research gap.
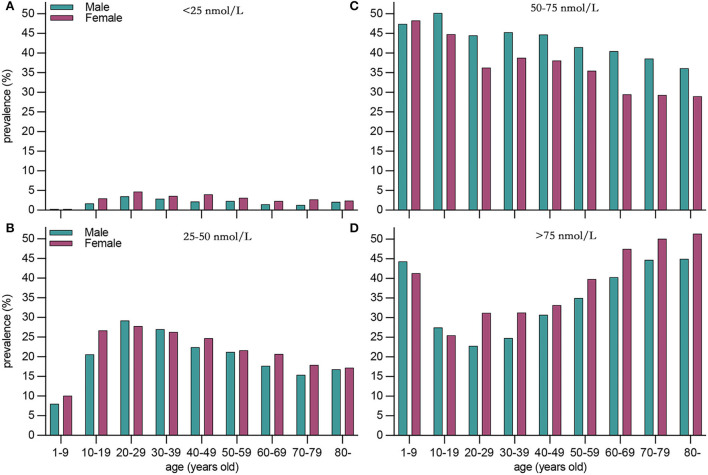
Methods: According to previous studies and nutritional guidelines for vitamin D, severe VDD was defined as serum 25(OH)D levels of <25 nmol/L, moderate deficiency as 25-50 nmol/L, insufficiency as 50-75 nmol/L, and sufficiency as >75 nmol/L. We comprehensively estimated the prevalence of serum 25(OH)D levels of <25, 25-50, 50-75, and >75 nmol/L in Americans and described trends in vitamin D status from 2001 to 2018. Weighted multivariate linear regression models were used to explore the predictors of VDD. All analyses and the data were adjusted for the complex sampling design of NHANES using Mobile Examination Center (MEC) weights.
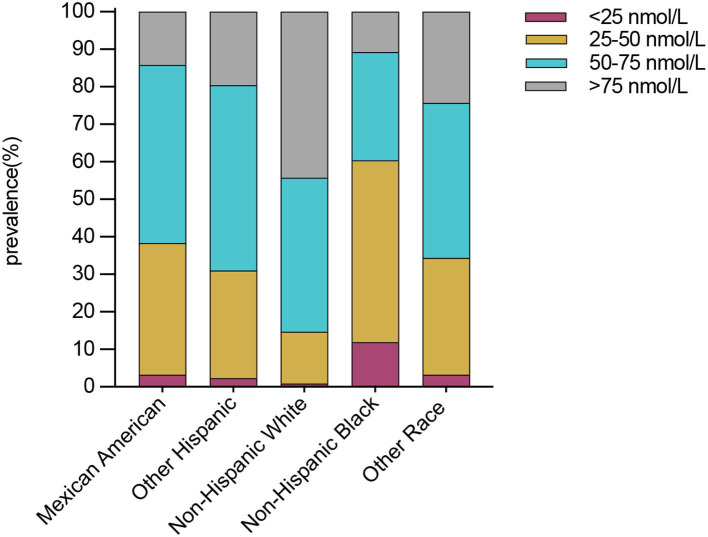
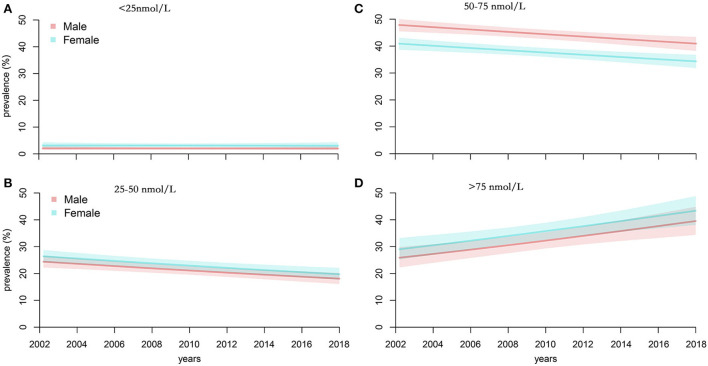
Results: Based on the most recent data of 71,685 participants, our study showed that the weighted prevalence of severe and moderate VDD was 2.6% and 22.0%, and the prevalence of vitamin D insufficiency (VDI) and sufficiency was 40.9% and 34.5%. The prevalence of severe and moderate VDD was higher in women, non-Hispanic black Americans, people aged 20-29 years, and during the season of winter. From 2001 to 2018, we found a slight linear decrease in the prevalence of moderate VDD (coefficient = -0.847; P = 0.009) and VDI (coefficient = -0.810; P = 0.014). We also found a slight linear increase in vitamin D sufficient (coefficient = 1.693; P = 0.004). However, no trend change was observed in severe VDD (coefficient = -0.037; P = 0.698). Age, sex, ethnicity, season, sun-protective behaviors, lower BMI, lower socioeconomic status (SES), drinking, and lower milk consumption were predictors of severe VDD.
Conclusion: Vitamin D deficiency is still prevalent in the United States, especially in non-Hispanic black Americans, women, individuals aged 20-29, and during winter. Therefore, individuals, healthcare providers, and policymakers should take public health measures to develop and implement prevention strategies to deal with VDD.
Keywords: NHANES; predictors; prevalence; trends; vitamin D.
Copyright © 2022 Cui, Xiao, Ma, Fan, Zhou, Zheng and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous