

Bleeding after percutaneous transhepatic biliary drainage due to arterial injury: A case study in patient with stable hemodynamic
- PMID: 36263331
- PMCID: PMC9574574
- DOI: 10.1016/j.radcr.2022.09.061
Bleeding after percutaneous transhepatic biliary drainage due to arterial injury: A case study in patient with stable hemodynamic
Abstract
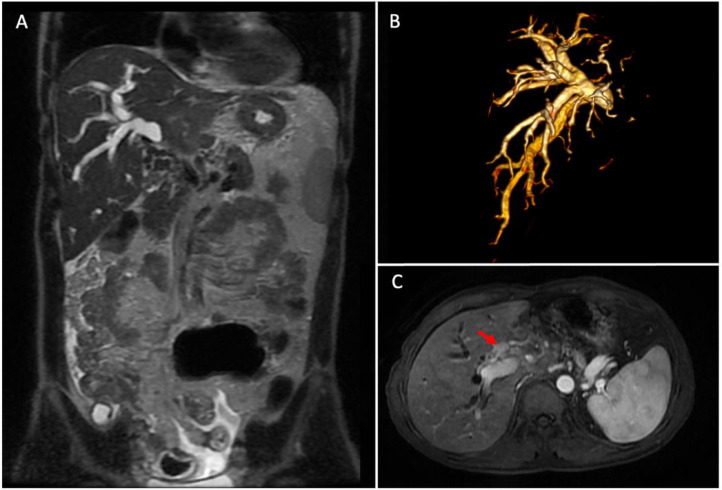
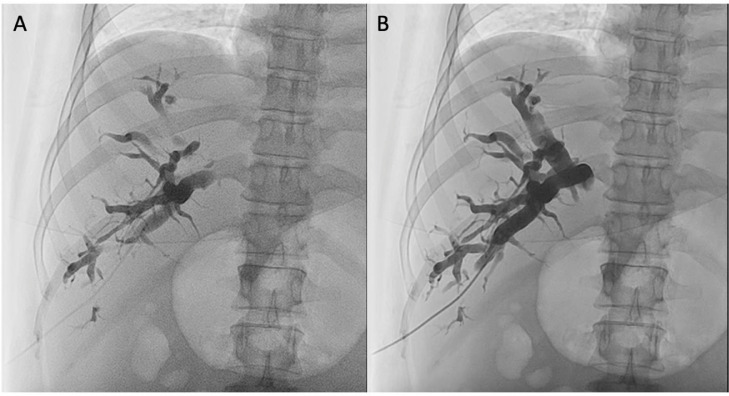
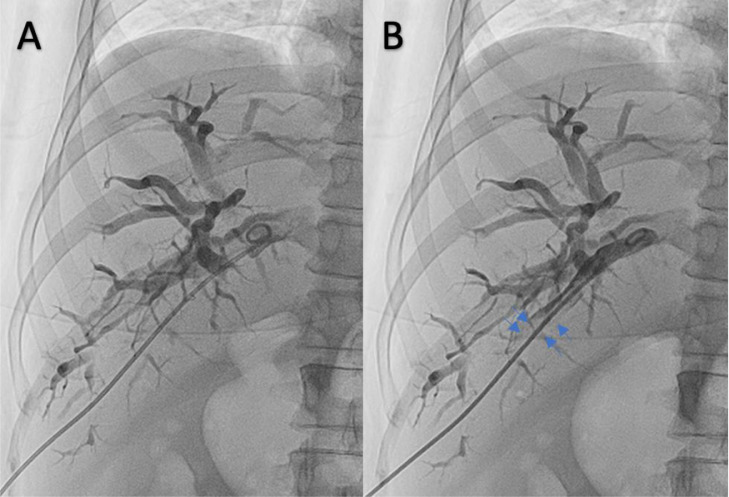
Percutaneous transhepatic biliary drainage (PTBD) is an effective procedure for correcting biliary obstructions. It can be performed under ultrasound and fluoroscopic equipment; however, it may entail serious complications, including bleeding, caused by arterial or venous injury. We present a 49-year-old man presented with a 1-month history of icterus, jaundice, dark urine, and right hypochondrial pain. MR imaging discovered a dilatation of the right intrahepatic bile duct due to obstruction by intrahepatic cholangiocarcinoma. PTBD procedure was performed in the right intrahepatic bile duct. After the pigtail drain device was inserted, the bile fluid color that came out from the pigtail turned sanguineous; nonetheless, the patient's hemodynamic was stable. Therefore, the second cholangiography was performed for evaluation. Some resistance was sensed during contrast injection into the bile duct, and the operator pushed the contrast media a little bit stronger and found a filling defect formed by a clot in the bile duct that suggested high suspicion of vessel injury. Although the patient's hemodynamics was still stable, the operator quickly decided to perform a hepatic arteriography procedure because bright red blood through the tube and a relatively rapid clot formed from the puncture point and distal drain, which were signs of hepatic artery injury. Hepatic arteriography confirmed the location of pseudoaneurysm caused by vessel trauma and arterio-intrahepatic bile duct fistulation. The embolization procedure was performed using PVA-300 into a ruptured hepatic artery branch through a microcatheter. Re-evaluation arteriography showed no pseudoaneurysm or arterio-intrahepatic bile duct fistulation after embolization.
Keywords: Arteriography; Cholangiography; Embolization; Percutaneous transhepatic biliary drainage.
© 2022 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures


References
-
- Houghton EJ, Invernizzi E, Acquafresca P, Palermo M, Giménez ME. Risk of bleeding complications in percutaneous biliary drainage: the paradox of the normal hemostasis. Arq Bras Cir Dig [Internet] 2019;32(3):e1454. http://www.ncbi.nlm.nih.gov/pubmed/31644674 Available from: - PMC - PubMed
-
- Pedersoli F, Schröder A, Zimmermann M, Schulze-Hagen M, Keil S, Ulmer TF, et al. Percutaneous transhepatic biliary drainage (PTBD) in patients with dilated vs. nondilated bile ducts: technical considerations and complications. Eur Radiol [Internet] 2021;31(5):3035–3041. http://www.ncbi.nlm.nih.gov/pubmed/33051733 Available from: - PMC - PubMed
-
- Quencer KB, Tadros AS, Marashi KB, Cizman Z, Reiner E, O'Hara R, et al. Bleeding after percutaneous transhepatic biliary drainage: incidence, causes and treatments. J Clin Med [Internet] 2018;7(5) http://www.ncbi.nlm.nih.gov/pubmed/29723964 Available from: - PMC - PubMed
-
- Saad WEA, Wallace MJ, Wojak JC, Kundu S, Cardella JF. Quality improvement guidelines for percutaneous transhepatic cholangiography, biliary drainage, and percutaneous cholecystostomy. J Vasc Interv Radiol [Internet] 2010;21(6):789–795. http://www.ncbi.nlm.nih.gov/pubmed/20307987 Available from: - PubMed
-
- Saad WEA, Davies MG, Darcy MD. Management of bleeding after percutaneous transhepatic cholangiography or transhepatic biliary drain placement. Tech Vasc Interv Radiol [Internet] 2008;11(1):60–71. https://linkinghub.elsevier.com/retrieve/pii/S1089251608000267 Available from: - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
