

Characterization of Errors in Retinopathy of Prematurity Diagnosis by Ophthalmologists-in-Training in Middle-Income Countries
- PMID: 36263934
- PMCID: PMC12309400
- DOI: 10.3928/01913913-20220609-02
Characterization of Errors in Retinopathy of Prematurity Diagnosis by Ophthalmologists-in-Training in Middle-Income Countries
Abstract
Purpose: To characterize common errors in the diagnosis of retinopathy of prematurity (ROP) among ophthalmologistsin-training in middle-income countries.
Methods: In this prospective cohort study, 200 ophthalmologists-in-training from programs in Brazil, Mexico, and the Philippines participated. A secure web-based educational system was developed using a repository of more than 2,500 unique image sets of ROP, and a reference standard diagnosis was established by combining the clinical diagnosis and the image-based diagnosis by multiple experts. Twenty web-based cases of wide-field retinal images were presented, and ophthalmologists-in-training were asked to diagnose plus disease, zone, stage, and category for each eye. Trainees' responses were compared to the consensus reference standard diagnosis. Main outcome measures were frequency and types of diagnostic errors were analyzed.
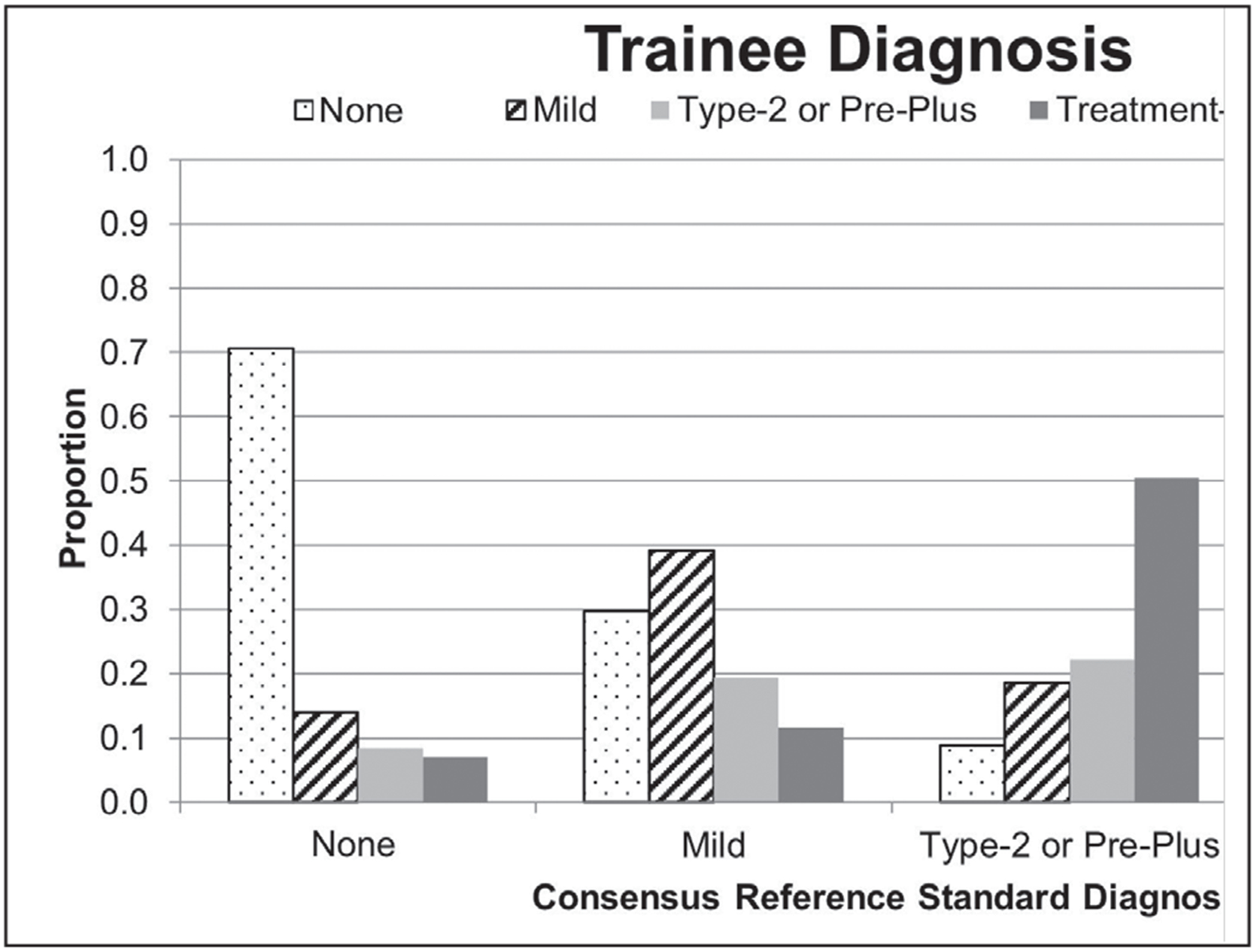
Results: The error rate in the diagnosis of any category of ROP was between 48% and 59% for all countries. The error rate in identifying type 2 or pre-plus disease was 77%, with a tendency for overdiagnosis (27% underdiagnosis vs 50% overdiagnosis; mean difference: 23.4; 95% CI: 12.1 to 34.7; P = .005). Misdiagnosis of treatment-requiring ROP as type 2 ROP was most commonly associated with incorrectly identifying plus disease (plus disease error rate = 18% with correct category diagnosis vs 69% when misdiagnosed; mean difference: 51.0; 95% CI: 49.3 to 52.7; P = .003).
Conclusions: Ophthalmologists-in-training from middle-income countries misdiagnosed ROP more than half of the time. Identification of plus disease was the salient factor leading to incorrect diagnosis. These findings emphasize the need for improved access to ROP education to improve competency in diagnosis among ophthalmologists-in-training in middle-income countries. [J Pediatr Ophthalmol Strabismus. 2023;60(5):344-352.].
Figures



References
Grants and funding
LinkOut - more resources
Full Text Sources