

Quantification and Proximal-to-Distal Distribution Pattern of Tibial Nerve Lesions in Relapsing-Remitting Multiple Sclerosis : Assessment by MR Neurography
- PMID: 36264352
- PMCID: PMC10219896
- DOI: 10.1007/s00062-022-01219-1
Quantification and Proximal-to-Distal Distribution Pattern of Tibial Nerve Lesions in Relapsing-Remitting Multiple Sclerosis : Assessment by MR Neurography
Abstract
Purpose: Recent studies suggest an involvement of the peripheral nervous system (PNS) in multiple sclerosis (MS). Here, we characterize the proximal-to-distal distribution pattern of peripheral nerve lesions in relapsing-remitting MS (RRMS) by quantitative magnetic resonance neurography (MRN).
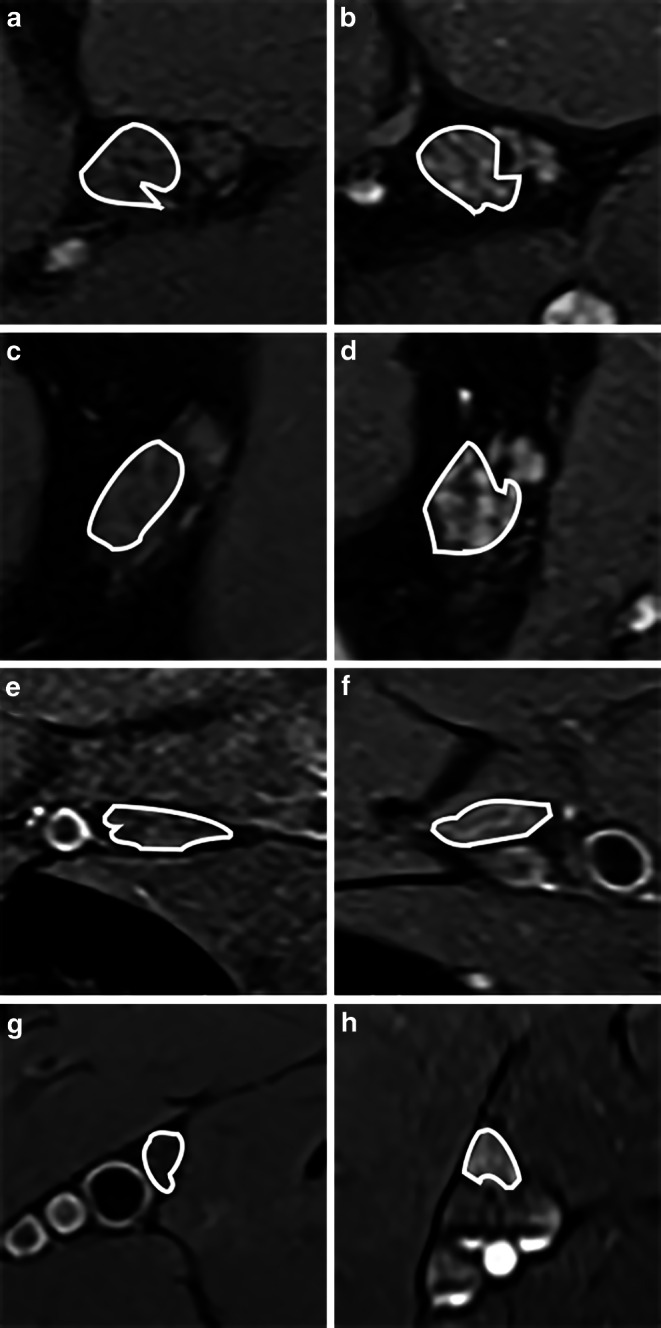
Methods: A total of 35 patients with RRMS were prospectively included and underwent detailed neurologic and electrophysiologic examinations. Additionally, 30 age- and sex-matched healthy controls were recruited. 3T MRN with anatomical coverage from the proximal thigh down to the tibiotalar joint was conducted using dual-echo 2‑dimensional relaxometry sequences with spectral fat saturation. Quantification of PNS involvement was performed by evaluating microstructural (proton spin density (ρ), T2-relaxation time (T2app)), and morphometric (cross-sectional area, CSA) MRN markers in every axial slice.
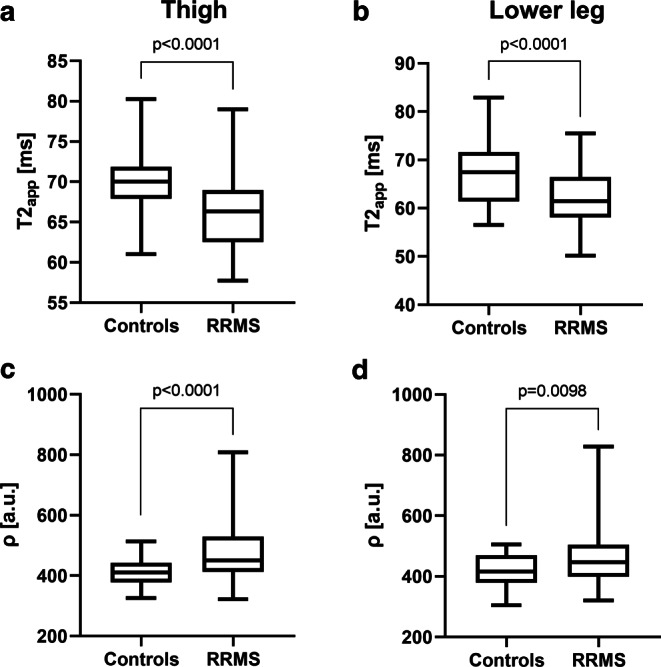
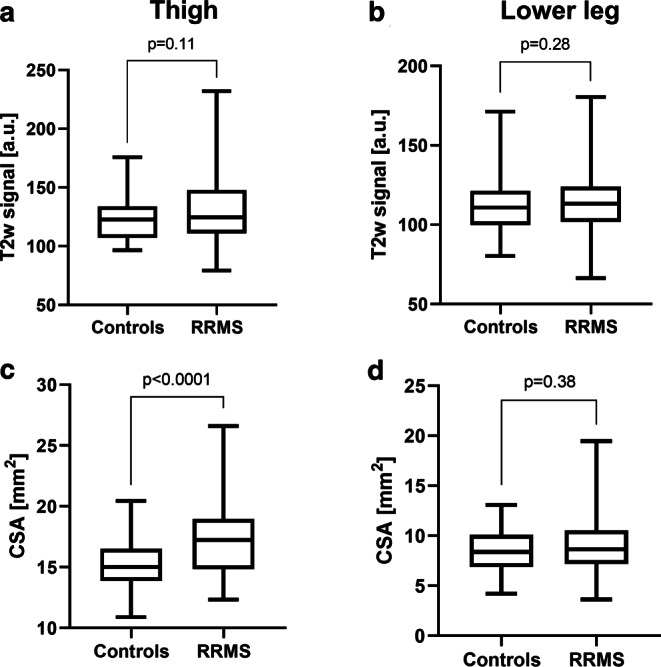
Results: In patients with RRMS, tibial nerve lesions at the thigh and the lower leg were characterized by a decrease in T2app and an increase in ρ compared to controls (T2app thigh: p < 0.0001, T2app lower leg: p = 0.0040; ρ thigh: p < 0.0001; ρ lower leg: p = 0.0098). An additional increase in nerve CSA was only detectable at the thigh, while the semi-quantitative marker T2w-signal was not altered in RRMS in both locations. A slight proximal-to-distal gradient was observed for T2app and T2-signal, but not for ρ.
Conclusion: PNS involvement in RRMS is characterized by a decrease in T2app and an increase in ρ, occurring with proximal predominance at the thigh and the lower leg. Our results indicate microstructural alterations in the extracellular matrix of peripheral nerves in RRMS and may contribute to a better understanding of the pathophysiologic relevance of PNS involvement.
Keywords: Magnetic resonance neurography; Peripheral nervous system; Proton spin density; Quantitative imaging markers; T2-relaxometry.
© 2022. The Author(s).
Conflict of interest statement
A. Viehöver received lecture honoraria from Roche and Merck. R. Diem received grants from the German Research Foundation (FOR 2289), the Hertie Foundation, and the German Ministry of Education and Research. M. Korporal-Kuhnke reports lecture honoraria from Novartis, BMS and Merck. O. Fösleitner received the Rahel Goetein-Straus stipend grant from the Medical Faculty of the University of Heidelberg. J.M.E. Jende received grants from the German Research Foundation (SFB 1158), and the International Foundation for Research in Paraplegia. S. Heiland received a research grant from the German Research Foundation (SFB 1118). B. Wildemann received grants from the German Ministry of Education and Research, German Research Foundation, Dietmar Hopp Foundation and Klaus Tschira Foundation, grants and personal fees from Merck, Sanofi Genzyme, Novartis, and personal fees from Alexion, Bayer, Biogen, Teva; none related to this work. M. Bendszus reports personal fees from Boehringer Ingelheim, grants and personal fees from Novartis, grants from Siemens, personal fees from Merck, personal fees from Bayer, grants and personal fees from Guerbet, grants from Hopp Foundation, grants from DFG, grants from European Union, grants from Stryker, personal fees from Teva, personal fees from BBraun, personal fees from Vascular Dynamics, personal fees from Grifols, personal fees from Neuroscios. J.C. Hayes received a research grant, personal fees, lecture honoraria and financial support for conference attendance from Alnylam Pharmaceuticals, the Olympia Morata stipend grant from the Medical Faculty of the University of Heidelberg, lecture honoraria and financial support for conference attendance from Pfizer, and advised for Akcea Therapeutics. A.M. Pietsch, M. Weiler, G. Sam and J.M. Hayes declare that they have no competing interests.
Figures
Similar articles
-
Peripheral Nerve Involvement in Friedreich's Ataxia Characterized by Quantitative Magnetic Resonance Neurography.Eur J Neurol. 2025 Mar;32(3):e70121. doi: 10.1111/ene.70121. Eur J Neurol. 2025. PMID: 40130461 Free PMC article.
-
Characterization and quantification of alcohol-related polyneuropathy by magnetic resonance neurography.Eur J Neurol. 2022 Feb;29(2):573-582. doi: 10.1111/ene.15127. Epub 2021 Oct 11. Eur J Neurol. 2022. PMID: 34564924
-
Peripheral nerve involvement in multiple sclerosis: Demonstration by magnetic resonance neurography.Ann Neurol. 2017 Nov;82(5):676-685. doi: 10.1002/ana.25068. Epub 2017 Oct 26. Ann Neurol. 2017. PMID: 29023976
-
[Clinical indications for high-resolution MRI diagnostics of the peripheral nervous system].Radiologe. 2017 Mar;57(3):148-156. doi: 10.1007/s00117-017-0210-6. Radiologe. 2017. PMID: 28188346 Review. German.
-
Peripheral nerve imaging in amyotrophic lateral sclerosis.Clin Neurophysiol. 2020 Sep;131(9):2315-2326. doi: 10.1016/j.clinph.2020.03.026. Epub 2020 Apr 13. Clin Neurophysiol. 2020. PMID: 32340815 Review.
Cited by
-
A Systematic Literature Review on Inflammatory Markers in the Saliva of Patients with Multiple Sclerosis: A Cause or a Consequence of Periodontal Diseases.Medicina (Kaunas). 2024 May 24;60(6):859. doi: 10.3390/medicina60060859. Medicina (Kaunas). 2024. PMID: 38929476 Free PMC article.
-
Quantitative magnetic resonance neurography in chronic inflammatory demyelinating polyradiculoneuropathy: A longitudinal study over 6 years.Ann Clin Transl Neurol. 2024 Mar;11(3):593-606. doi: 10.1002/acn3.51978. Epub 2023 Dec 19. Ann Clin Transl Neurol. 2024. PMID: 38111964 Free PMC article.
-
Peripheral Nerve Involvement in Friedreich's Ataxia Characterized by Quantitative Magnetic Resonance Neurography.Eur J Neurol. 2025 Mar;32(3):e70121. doi: 10.1111/ene.70121. Eur J Neurol. 2025. PMID: 40130461 Free PMC article.
-
Evolution of peripheral nerve changes in early multiple sclerosis-a longitudinal MR neurography study.Front Neurol. 2024 May 3;15:1335408. doi: 10.3389/fneur.2024.1335408. eCollection 2024. Front Neurol. 2024. PMID: 38765263 Free PMC article.
-
Automated peripheral nerve segmentation for MR-neurography.Eur Radiol Exp. 2024 Aug 26;8(1):97. doi: 10.1186/s41747-024-00503-8. Eur Radiol Exp. 2024. PMID: 39186183 Free PMC article.
References
-
- Hoffmann S, Vitzthum K, Mache S, Spallek M. Multiple Sklerose: Epidemiologie, Pathophysiologie, Diagnostik und Therapie. Prakt Arb Med. 2009;17:12–18.
-
- Fischer M, Kunkel A, Bublak P, Faiss JH, Hoffmann F, Sailer M, Schwab M, Zettl UK, Köhler W. How reliable is the classification of cognitive impairment across different criteria in early and late stages of multiple sclerosis? J Neurol Sci. 2014;343:91–99. doi: 10.1016/j.jns.2014.05.042. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
