

Imaging assessment after pancreaticoduodenectomy: reconstruction techniques-normal findings and complications
- PMID: 36264369
- PMCID: PMC9584030
- DOI: 10.1186/s13244-022-01306-4
Imaging assessment after pancreaticoduodenectomy: reconstruction techniques-normal findings and complications
Abstract
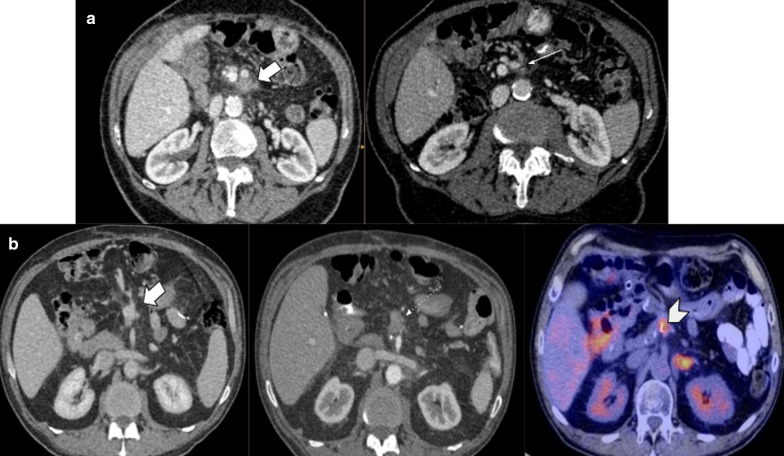
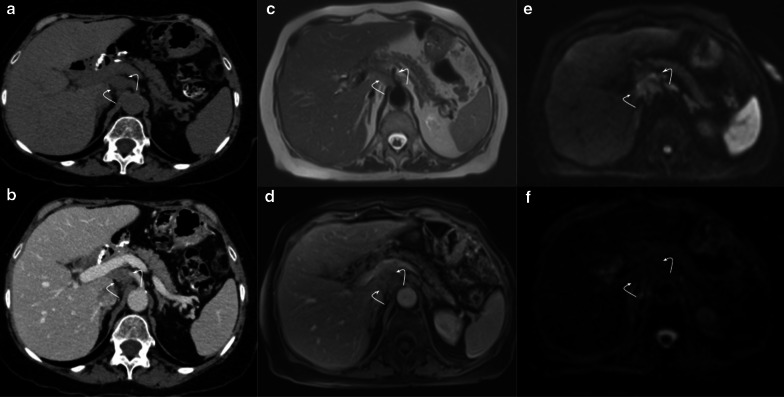
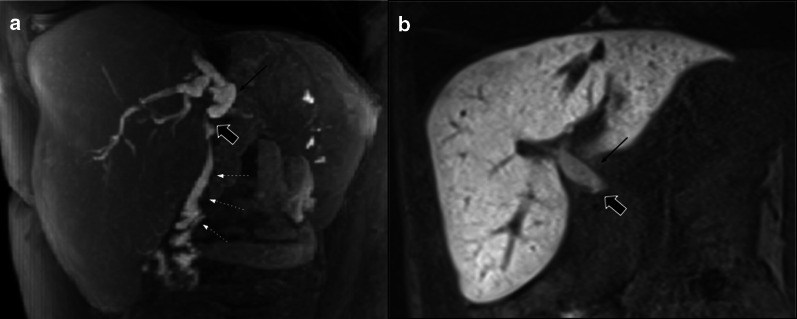
Pancreaticoduodenectomy represents a major surgery for tumors located at the pancreatic head and the ampullary/periampullary region. This complex procedure is associated with a high morbidity rate. Many surgical techniques have been proposed in order to reduce mortality rates, although post-procedure complications represent a current problem. Different imaging findings and complications may appear depending on the surgical technique used. Hence, radiologists should be familiarized with them to distinguish normal findings from real complications. The most challenging scenarios are represented by abdominal fluid collections, and tumor recurrence, that may frequently mimic normal postsurgical changes.
Keywords: Hepaticojejunostomy; Pancreatic cancer; Pancreatic fistula; Pancreaticoduodenectomy; Pancreaticojejunostomy.
© 2022. The Author(s).
Conflict of interest statement
The authors of this study have no competing interests.
Figures

























References
-
- (2018) Whipple procedure. AORN J 108(5):P11–P13 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
