

Retrospective evaluation of national MRI reporting quality for lateral lymph nodes in rectal cancer patients and concordance with prospective re-evaluation following additional training
- PMID: 36264440
- PMCID: PMC9583997
- DOI: 10.1186/s13244-022-01303-7
Retrospective evaluation of national MRI reporting quality for lateral lymph nodes in rectal cancer patients and concordance with prospective re-evaluation following additional training
Abstract
Objectives: The presence and size of lateral lymph nodes (LLNs) are important factors influencing treatment decisions for rectal cancer. Awareness of the clinical relevance and describing LLNs in MRI reports is therefore essential. This study assessed whether LLNs were mentioned in primary MRI reports at a national level and investigated the concordance with standardised re-review.
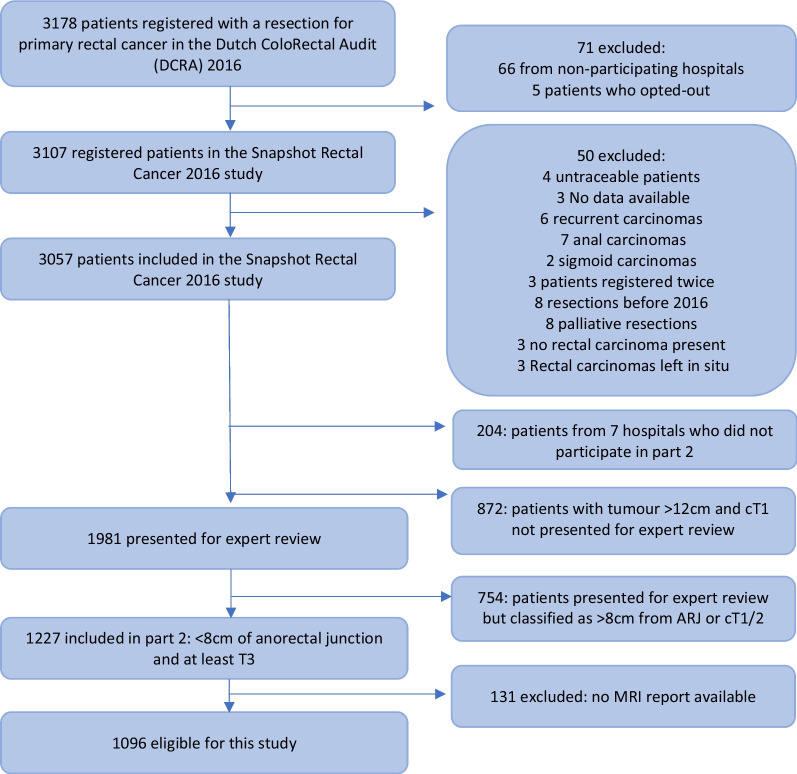
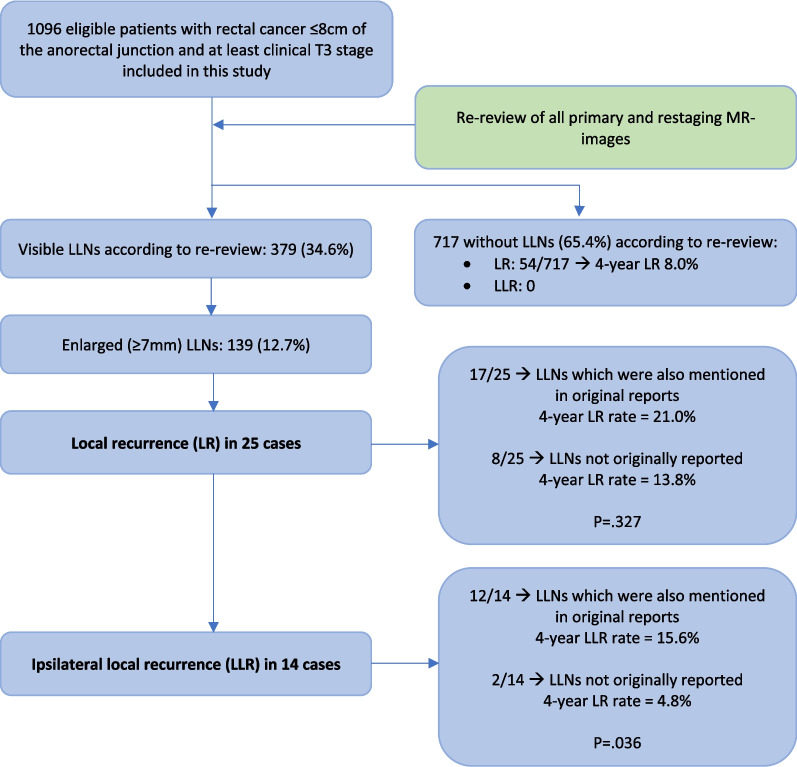
Methods: This national, retrospective, cross-sectional cohort study included 1096 patients from 60 hospitals treated in 2016 for primary cT3-4 rectal cancer ≤ 8 cm from the anorectal junction. Abdominal radiologists re-reviewed all MR images following a 2-h training regarding LLNs.
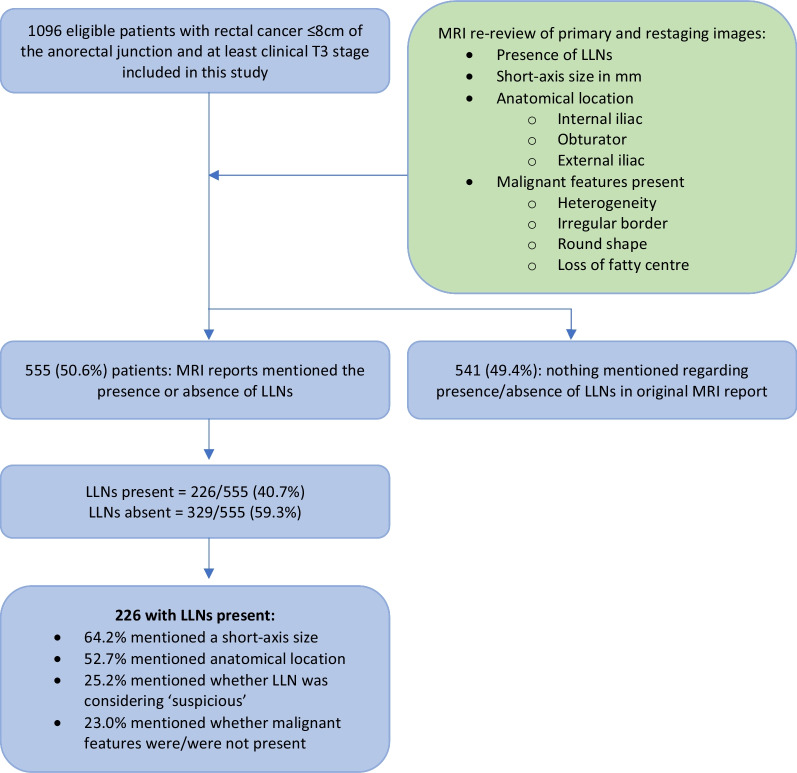
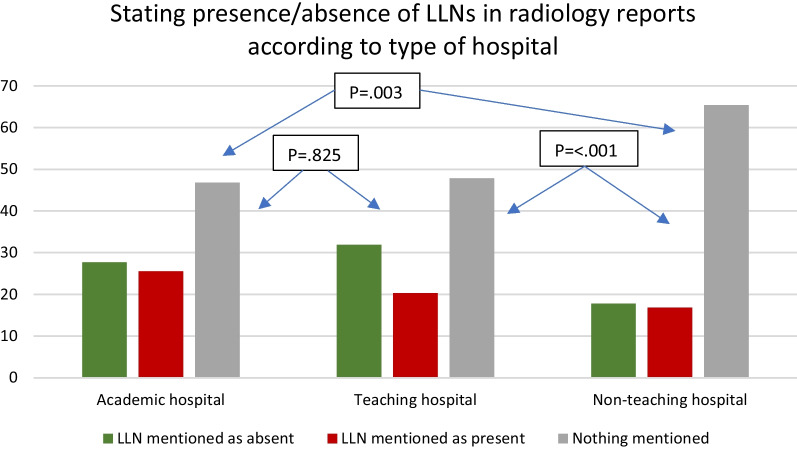
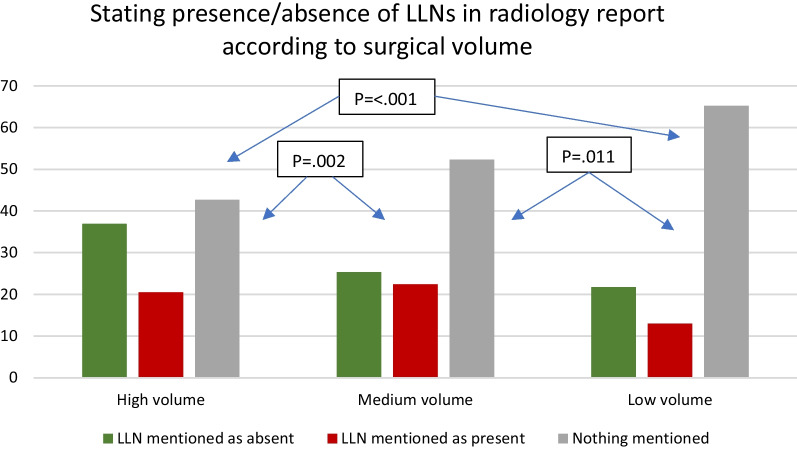
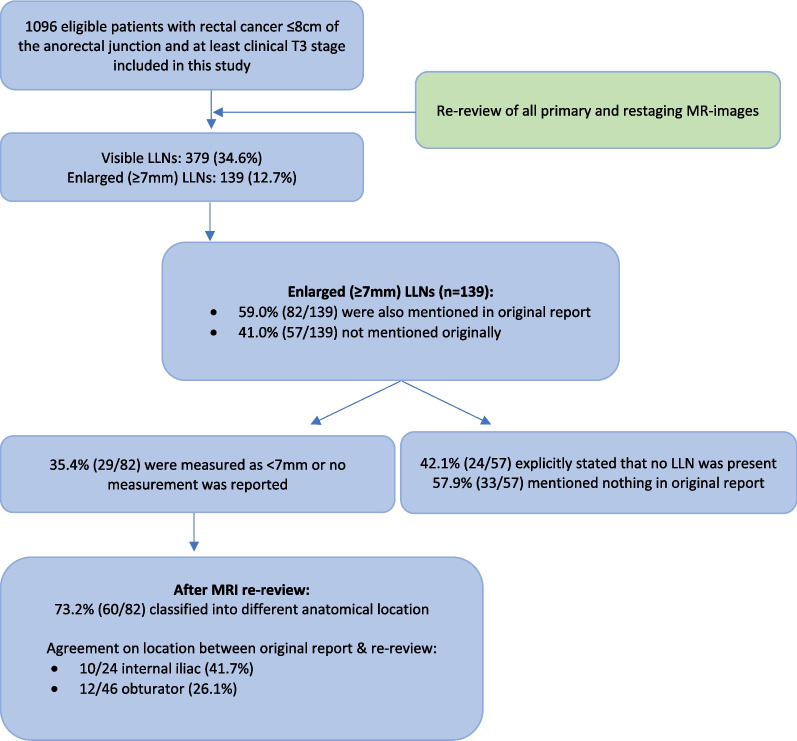
Results: Re-review of MR images identified that 41.0% of enlarged (≥ 7 mm) LLNs were not mentioned in primary MRI reports. A contradictory anatomical location was stated for 73.2% of all LLNs and a different size (≥/< 7 mm) for 41.7%. In total, 49.4% of all cases did not mention LLNs in primary MRI reports. Reporting LLNs was associated with stage (cT3N0 44.3%, T3N+/T4 52.8%, p = 0.013), cN stage (N0 44.1%, N1 48.6%, N2 59.5%, p < 0.001), hospital type (non-teaching 34.6%, teaching 52.2%, academic 53.2% p = 0.006) and annual rectal cancer resection volumes (low 34.8%, medium 47.7%, high 57.3% p < 0.001). For LLNs present according to original MRI reports (n = 226), 64.2% also mentioned a short-axis size, 52.7% an anatomical location and 25.2% whether it was deemed suspicious.
Conclusions: Almost half of the primary MRI reports for rectal cancer patients treated in the Netherlands in 2016 did not mention LLNs. A significant portion of enlarged LLNs identified during re-review were also not mentioned originally, with considerable discrepancies for location and size. These results imply insufficient awareness and indicate the need for templates, education and training.
Keywords: Lateral lymph nodes; MR imaging; Rectal cancer.
© 2022. The Author(s).
Conflict of interest statement
RBT is a member of the Insights into Imaging Advisory Editorial Board. She has not taken part in the review or selection process of this article. The remaining authors declare that they have no competing interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
