

Integrated host-microbe plasma metagenomics for sepsis diagnosis in a prospective cohort of critically ill adults
- PMID: 36266337
- PMCID: PMC9613463
- DOI: 10.1038/s41564-022-01237-2
Integrated host-microbe plasma metagenomics for sepsis diagnosis in a prospective cohort of critically ill adults
Abstract
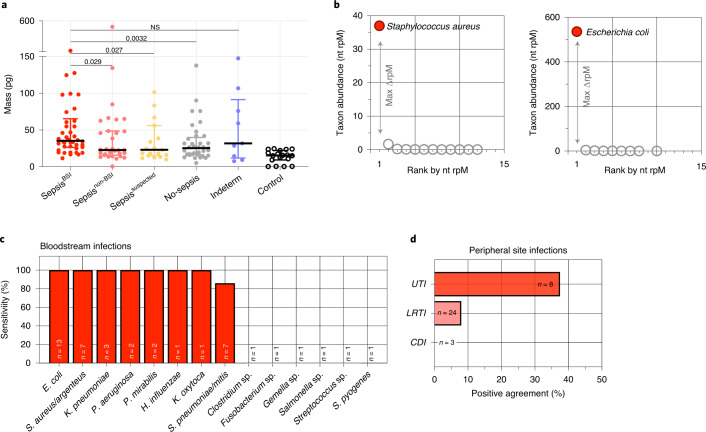
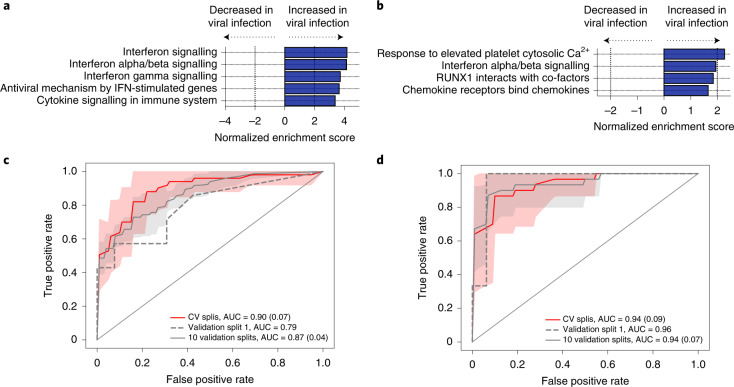
We carried out integrated host and pathogen metagenomic RNA and DNA next generation sequencing (mNGS) of whole blood (n = 221) and plasma (n = 138) from critically ill patients following hospital admission. We assigned patients into sepsis groups on the basis of clinical and microbiological criteria. From whole-blood gene expression data, we distinguished patients with sepsis from patients with non-infectious systemic inflammatory conditions using a trained bagged support vector machine (bSVM) classifier (area under the receiver operating characteristic curve (AUC) = 0.81 in the training set; AUC = 0.82 in a held-out validation set). Plasma RNA also yielded a transcriptional signature of sepsis with several genes previously reported as sepsis biomarkers, and a bSVM sepsis diagnostic classifier (AUC = 0.97 training set; AUC = 0.77 validation set). Pathogen detection performance of plasma mNGS varied on the basis of pathogen and site of infection. To improve detection of virus, we developed a secondary transcriptomic classifier (AUC = 0.94 training set; AUC = 0.96 validation set). We combined host and microbial features to develop an integrated sepsis diagnostic model that identified 99% of microbiologically confirmed sepsis cases, and predicted sepsis in 74% of suspected and 89% of indeterminate sepsis cases. In summary, we suggest that integrating host transcriptional profiling and broad-range metagenomic pathogen detection from nucleic acid is a promising tool for sepsis diagnosis.
© 2022. The Author(s).
Conflict of interest statement
C.R.L., K.L.K., L.N. and C.S.C. are inventors on a provisional patent (no. 63/342,528) related to the methodology. The authors declare no other competing interests.
Figures





Comment in
-
Combining pathogen and host metagenomics for a better sepsis diagnostic.Nat Microbiol. 2022 Nov;7(11):1713-1714. doi: 10.1038/s41564-022-01255-0. Nat Microbiol. 2022. PMID: 36289401 No abstract available.
References
-
- Liu V, et al. Hospital deaths in patients with sepsis from 2 independent cohorts. JAMA. 2014;312:90–92. - PubMed
-
- Ferrer R, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit. Care Med. 2014;42:1749–1755. - PubMed
-
- Novosad SA, et al. Vital signs: epidemiology of sepsis: prevalence of health care factors and opportunities for prevention. MMWR Morb. Mortal. Wkly Rep. 2016;65:864–869. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
