

A systematic review and meta-analysis on delaying surgery for urothelial carcinoma of bladder and upper tract urothelial carcinoma: Implications for the COVID19 pandemic and beyond
- PMID: 36268209
- PMCID: PMC9577485
- DOI: 10.3389/fsurg.2022.879774
A systematic review and meta-analysis on delaying surgery for urothelial carcinoma of bladder and upper tract urothelial carcinoma: Implications for the COVID19 pandemic and beyond
Abstract
Purpose: The COVID-19 pandemic has led to competing strains on hospital resources and healthcare personnel. Patients with newly diagnosed invasive urothelial carcinomas of bladder (UCB) upper tract (UTUC) may experience delays to definitive radical cystectomy (RC) or radical nephro-ureterectomy (RNU) respectively. We evaluate the impact of delaying definitive surgery on survival outcomes for invasive UCB and UTUC.
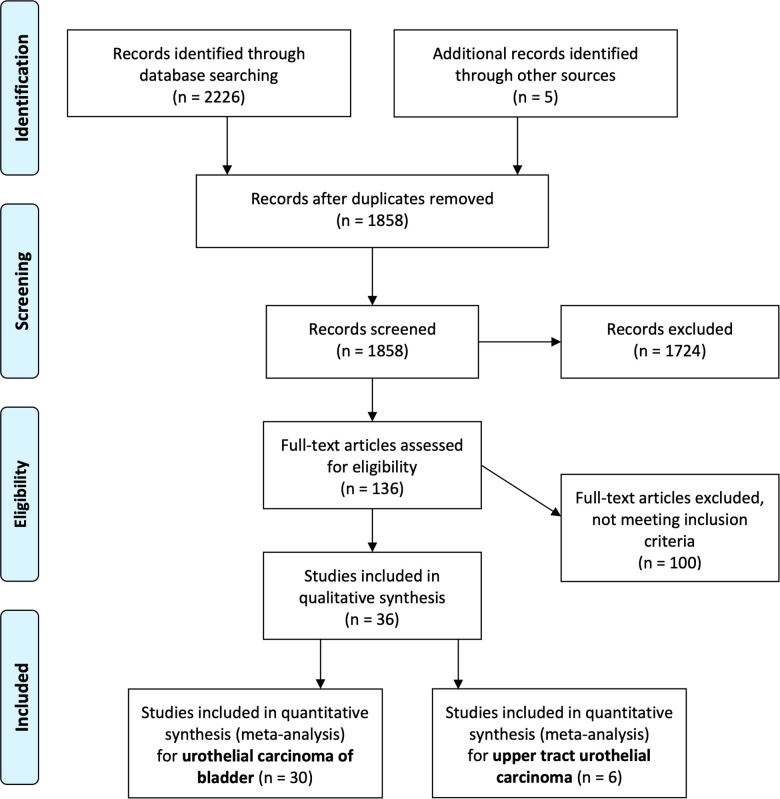
Methods: We searched for all studies investigating delayed urologic cancer surgery in Medline and Embase up to June 2020. A systematic review and meta-analysis was performed.
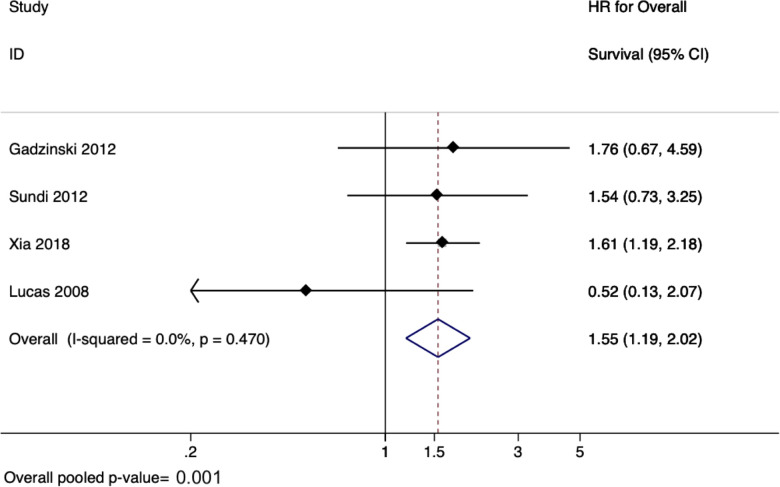
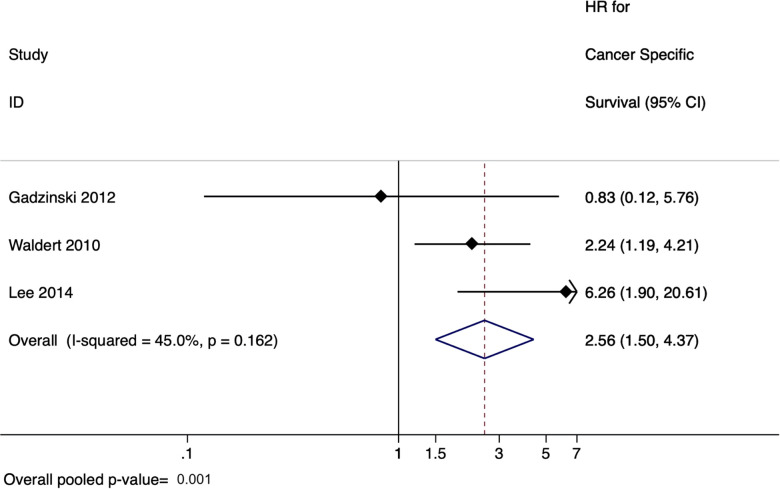
Results: We identified a total of 30 studies with 32,591 patients. Across 13 studies (n = 12,201), a delay from diagnosis of bladder cancer/TURBT to RC was associated with poorer overall survival (HR 1.25, 95% CI: 1.09-1.45, p = 0.002). For patients who underwent neoadjuvant chemotherapy before RC, across the 5 studies (n = 4,316 patients), a delay between neoadjuvant chemotherapy and radical cystectomy was not found to be significantly associated with overall survival (pooled HR 1.37, 95% CI: 0.96-1.94, p = 0.08). For UTUC, 6 studies (n = 4,629) found that delay between diagnosis of UTUC to RNU was associated with poorer overall survival (pooled HR 1.55, 95% CI: 1.19-2.02, p = 0.001) and cancer-specific survival (pooled HR of 2.56, 95% CI: 1.50-4.37, p = 0.001). Limitations included between-study heterogeneity, particularly in the definitions of delay cut-off periods between diagnosis to surgery.
Conclusions: A delay from diagnosis of UCB or UTUC to definitive RC or RNU was associated with poorer survival outcomes. This was not the case for patients who received neoadjuvant chemotherapy.
Keywords: bladder cancer; bladder carcinoma; delay in surgery; delayed treatment; time-to-treatment; ureteral neoplasms; urinary bladder neoplasms; urothelial carcinoma.
© 2022 Leow, Tan, Tan, Tan, Chan, Tikkinen, Kamat, Sengupta, Meng, Shariat, Roupret, Decaestecker, Vasdev, Chong, Enikeev, Giannarini, Ficarra and Teoh.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Neoadjuvant and Adjuvant Chemotherapy for Upper Tract Urothelial Carcinoma: A 2020 Systematic Review and Meta-analysis, and Future Perspectives on Systemic Therapy.Eur Urol. 2021 May;79(5):635-654. doi: 10.1016/j.eururo.2020.07.003. Epub 2020 Aug 12. Eur Urol. 2021. PMID: 32798146
-
Stage-specific impact of tumor location on oncologic outcomes in patients with upper and lower tract urothelial carcinoma following radical surgery.Eur Urol. 2012 Oct;62(4):677-84. doi: 10.1016/j.eururo.2012.02.018. Epub 2012 Feb 15. Eur Urol. 2012. PMID: 22349570
-
Oncological Outcomes of Laparoscopic Nephroureterectomy Versus Open Radical Nephroureterectomy for Upper Tract Urothelial Carcinoma: An European Association of Urology Guidelines Systematic Review.Eur Urol Focus. 2019 Mar;5(2):205-223. doi: 10.1016/j.euf.2017.10.003. Epub 2017 Nov 15. Eur Urol Focus. 2019. PMID: 29154042
-
Aristolochic acid-associated urinary tract cancers: an updated meta-analysis of risk and oncologic outcomes after surgery and systematic review of molecular alterations observed in human studies.Ther Adv Drug Saf. 2021 Mar 21;12:2042098621997727. doi: 10.1177/2042098621997727. eCollection 2021. Ther Adv Drug Saf. 2021. PMID: 33815744 Free PMC article.
-
The Impact of Surgical Waiting Time on Oncological Outcomes in Patients with Upper Tract Urothelial Carcinoma Undergoing Radical Nephroureterectomy: A Systematic Review.J Clin Med. 2022 Jul 11;11(14):4007. doi: 10.3390/jcm11144007. J Clin Med. 2022. PMID: 35887771 Free PMC article. Review.
Cited by
-
Association between time to treatment and bladder cancer survival: a population-based analysis.Transl Androl Urol. 2024 Sep 30;13(9):2079-2091. doi: 10.21037/tau-24-148. Epub 2024 Sep 26. Transl Androl Urol. 2024. PMID: 39434744 Free PMC article.
-
A Retrospective Analysis of the Challenges of Urothelial Cancer Management during the COVID-19 Pandemic at a Single Academic Center in Romania.Healthcare (Basel). 2023 Mar 9;11(6):812. doi: 10.3390/healthcare11060812. Healthcare (Basel). 2023. PMID: 36981469 Free PMC article.
-
Can We Identify Patients in Danger of Delayed Treatment? Management of COVID-19 Pandemic Backlog in Urology Care in Poland.Int J Environ Res Public Health. 2022 Dec 9;19(24):16547. doi: 10.3390/ijerph192416547. Int J Environ Res Public Health. 2022. PMID: 36554427 Free PMC article.
-
Economic impact of reduced postoperative visits after inflatable penile prosthesis implantation.J Comp Eff Res. 2025 Mar;14(3):e240204. doi: 10.57264/cer-2024-0204. Epub 2025 Jan 15. J Comp Eff Res. 2025. PMID: 39812079 Free PMC article.
-
Pandemic Stressors and Adaptive Responses: A Longitudinal Analysis of the Quality of Life and Psychosocial Dynamics among Urothelial Cancer Patients.J Pers Med. 2023 Oct 28;13(11):1547. doi: 10.3390/jpm13111547. J Pers Med. 2023. PMID: 38003862 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources