

Left-atrial long-axis shortening allows effective quantification of atrial function and optimized risk prediction following acute myocardial infarction
- PMID: 36268539
- PMCID: PMC9574426
- DOI: 10.1093/ehjopen/oeac053
Left-atrial long-axis shortening allows effective quantification of atrial function and optimized risk prediction following acute myocardial infarction
Abstract
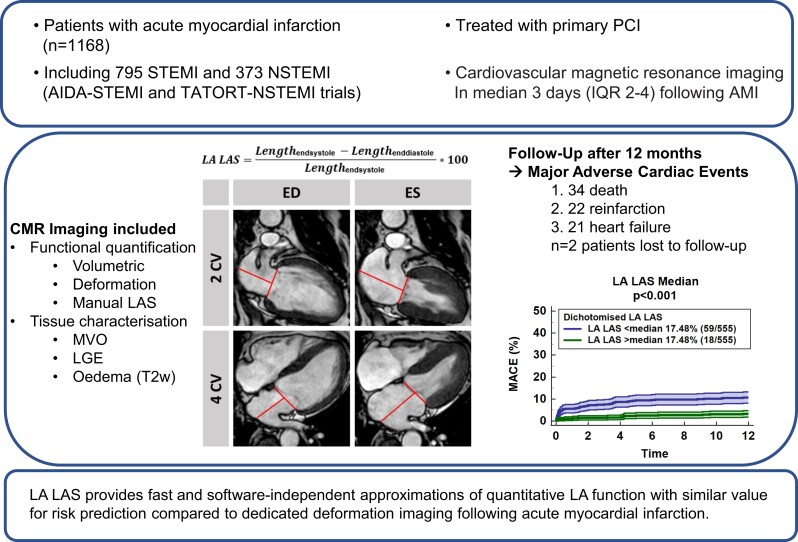
Aims: Deformation imaging enables optimized risk prediction following acute myocardial infarction (AMI). However, costly and time-consuming post processing has hindered widespread clinical implementation. Since manual left-ventricular long-axis strain (LV LAS) has been successfully proposed as a simple alternative for LV deformation imaging, we aimed at the validation of left-atrial (LA) LAS.
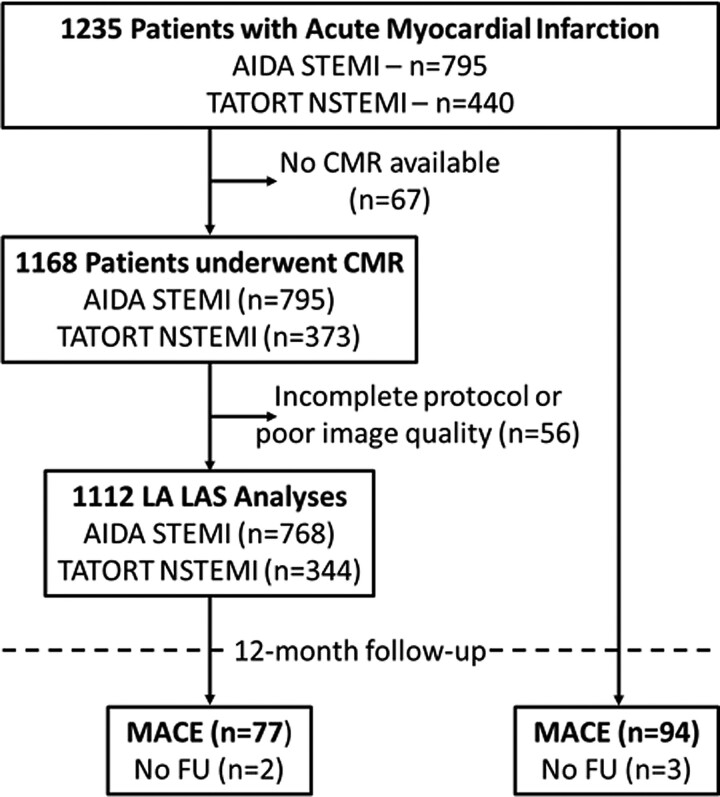
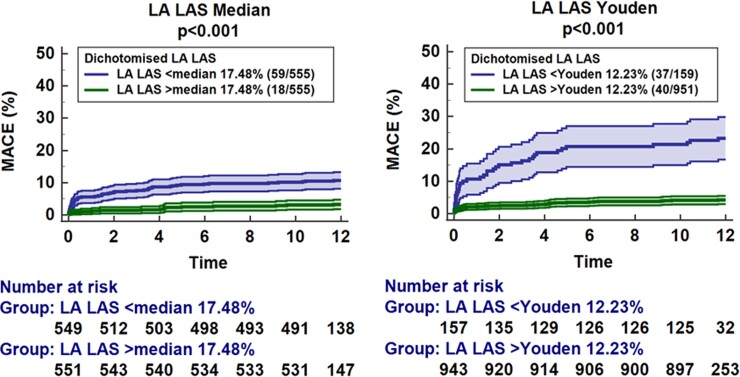
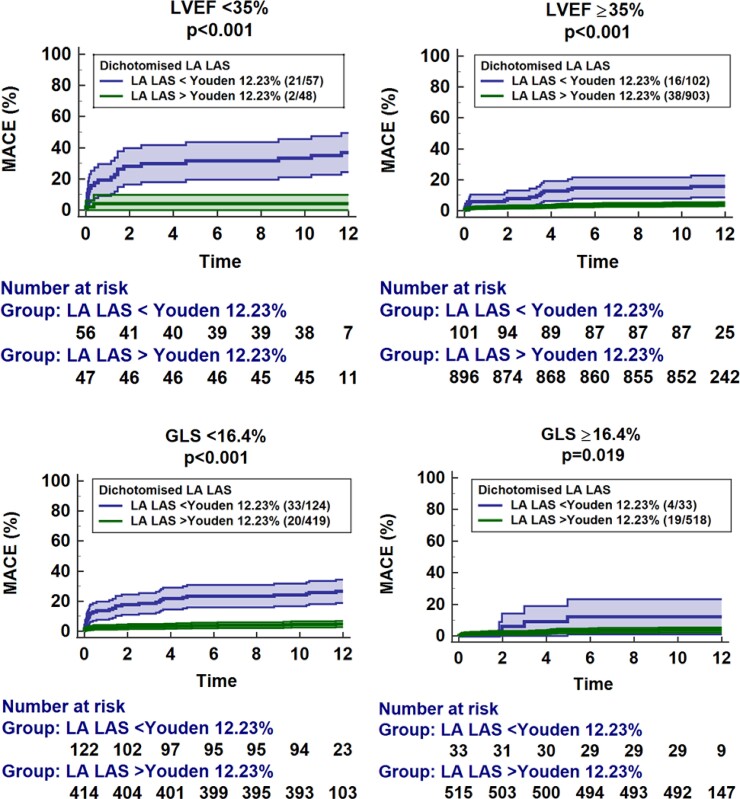
Methods and results: The AIDA STEMI and TATORT-NSTEMI trials recruited 795 patients with ST-elevation myocardial infarction and 440 with non-ST-elevation myocardial infarction. LA LAS was assessed as the systolic distance change between the middle of a line connecting the origins of the mitral leaflets and either a perpendicular line towards the posterior atrial wall (LAS90) or a line connecting to the LA posterior portion of the greatest distance irrespective of a predefined angle (LAS). Primary endpoint was major adverse cardiac event (MACE) occurrence within 12 months. There were no significant differences between LA LAS and LAS90, both with excellent reproducibility. LA LAS correlated significantly with LA reservoir function (Es, r = 0.60, P < 0.001). Impaired LA LAS resulted in higher MACE occurrence [hazard ratio (HR) 0.85, 95% confidence interval (CI) 0.82-0.88, P < 0.001]. LA LAS (HR 0.90, 95% CI 0.83-0.97, P = 0.005) and LV global longitudinal strain (GLS, P = 0.025) were the only independent predictors for MACE in multivariate analyses. C-statistics demonstrated incremental value of LA LAS in addition to GLS (P = 0.016) and non-inferiority compared with FT Es (area under the receiver operating characteristic curve 0.74 vs. 0.69, P = 0.256).
Conclusion: Left-atrial LAS provides fast and software-independent approximations of quantitative LA function with similar value for risk prediction compared with dedicated deformation imaging.
Clinical trial registration: ClinicalTrials.gov: NCT00712101 and NCT01612312.
Keywords: Atrial physiology; Left-atrial long-axis strain; Myocardial infarction; Prognosis.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures

References
-
- Smith SC, Collins A, Ferrari R, Holmes DR, Logstrup S, McGhie DV, Ralston J, Sacco RL, Stam H, Taubert K, Wood DA, Zoghbi WA. Our time: a call to save preventable death from cardiovascular disease (heart disease and stroke). Circulation 2012;126:2769–2775. - PubMed
-
- Roffi M, Patrono C, Collet J-P, Mueller C, Valgimigli M, Andreotti F, Bax JJ, Borger MA, Brotons C, Chew DP, Gencer B, Hasenfuss G, Kjeldsen K, Lancellotti P, Landmesser U, Mehilli J, Mukherjee D, Storey RF, Windecker S, ESC Scientific Document Group . 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: task force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J 2016;37:267–315. - PubMed
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, Caforio ALP, Crea F, Goudevenos JA, Halvorsen S, Hindricks G, Kastrati A, Lenzen MJ, Prescott E, Roffi M, Valgimigli M, Varenhorst C, Vranckx P, Widimský P, ESC Scientific Document Group . 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J 2018;39:119–177. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González-Juanatey JR, Harjola V-P, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P, Authors/Task Force Members; Document Reviewers . 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016;37:2129–2200. - PubMed
-
- White HD, Norris RM, Brown MA, Brandt PW, Whitlock RM, Wild CJ. Left ventricular end-systolic volume as the major determinant of survival after recovery from myocardial infarction. Circulation 1987;76:44–51. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
