

Positron Emission Tomography-Adapted Therapy in Bulky Stage I/II Classic Hodgkin Lymphoma: CALGB 50801 (Alliance)
- PMID: 36269899
- PMCID: PMC9928671
- DOI: 10.1200/JCO.22.00947
Positron Emission Tomography-Adapted Therapy in Bulky Stage I/II Classic Hodgkin Lymphoma: CALGB 50801 (Alliance)
Abstract
Purpose: Patients with bulky stage I/II classic Hodgkin lymphoma (cHL) are typically treated with chemotherapy followed by radiation. Late effects associated with radiotherapy include increased risk of second cancer and cardiovascular disease. We tested a positron emission tomography (PET)-adapted approach in patients with bulky, early-stage cHL, omitting radiotherapy in patients with interim PET-negative (PET-) disease and intensifying treatment in patients with PET-positive (PET+) disease.
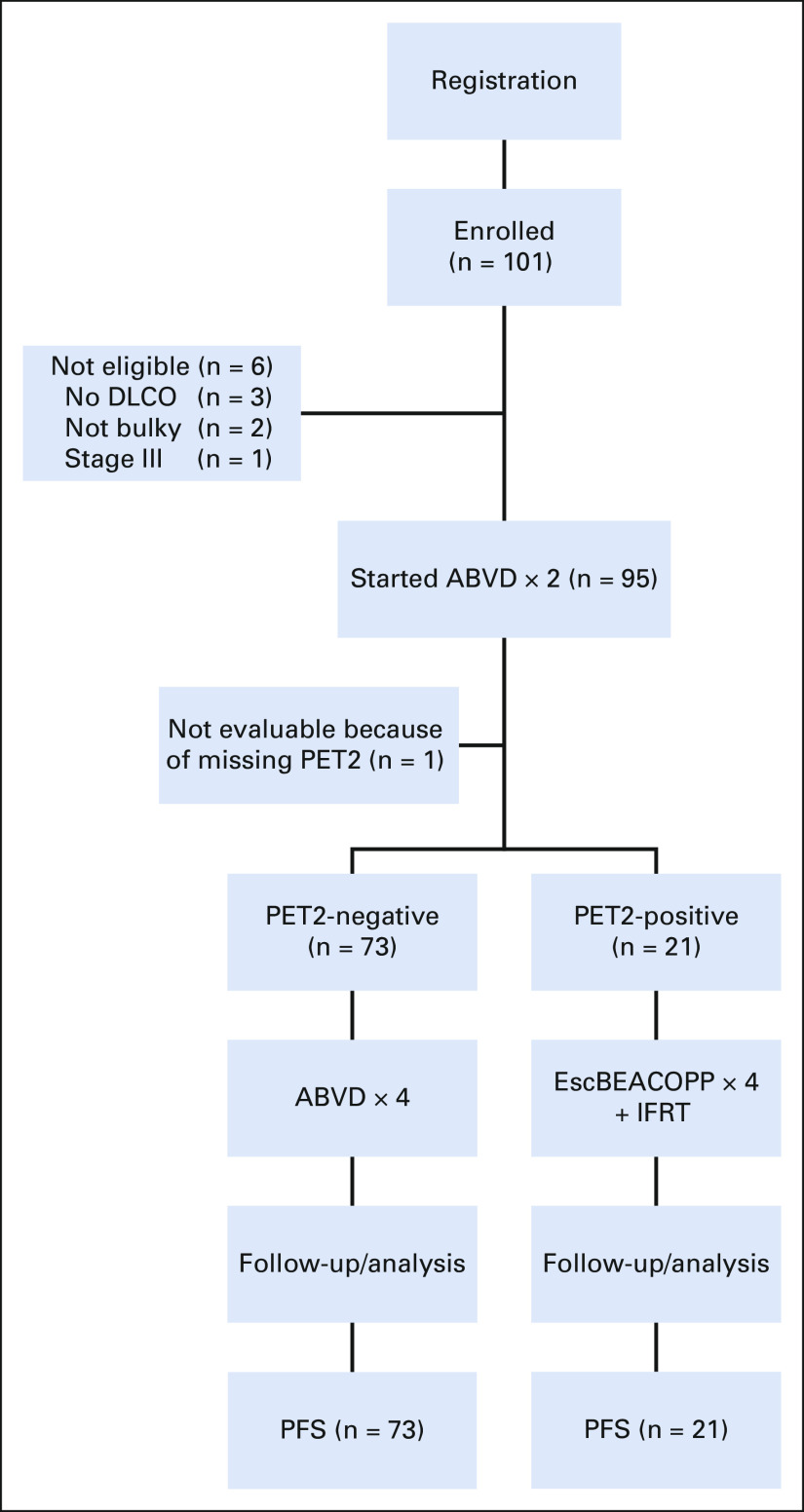
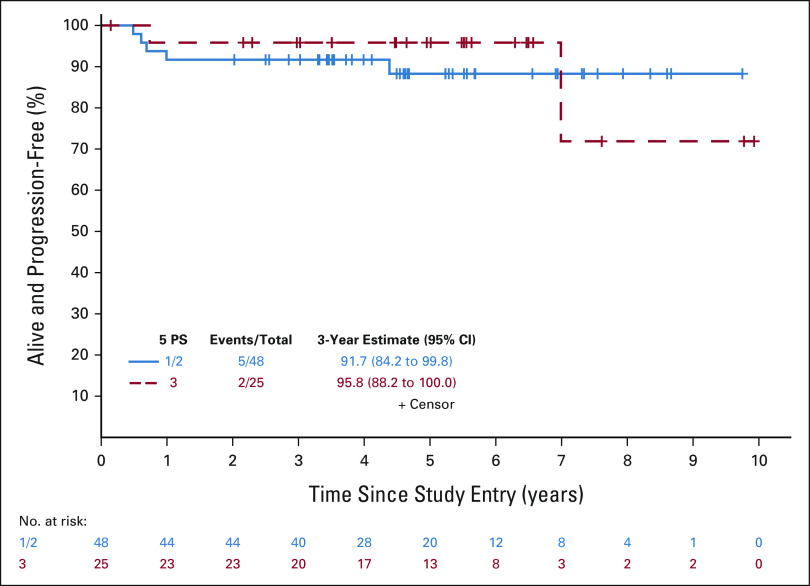
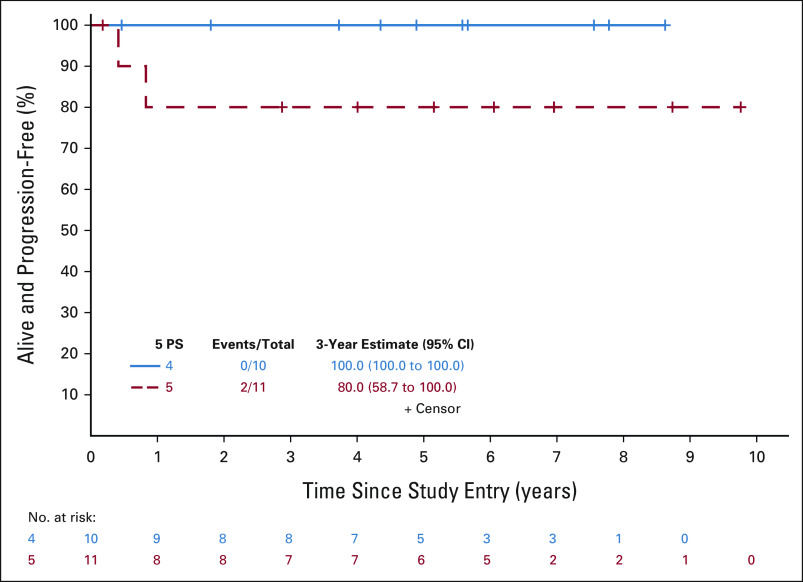
Methods: Eligible patients with bulky disease (mass > 10 cm or 1/3 the maximum intrathoracic diameter on chest x-ray) received two cycles of doxorubicin, bleomycin, vinblastine, and dacarbazine (ABVD) followed by interim fluorodeoxyglucose PET (PET2). Patients with PET2-, defined as 1-3 on the 5-point scale, received four additional cycles of doxorubicin, bleomycin, vinblastine, and dacarbazine. Patients with PET2+ received four cycles of escalated bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone followed by 30.6 Gy involved-field radiation.
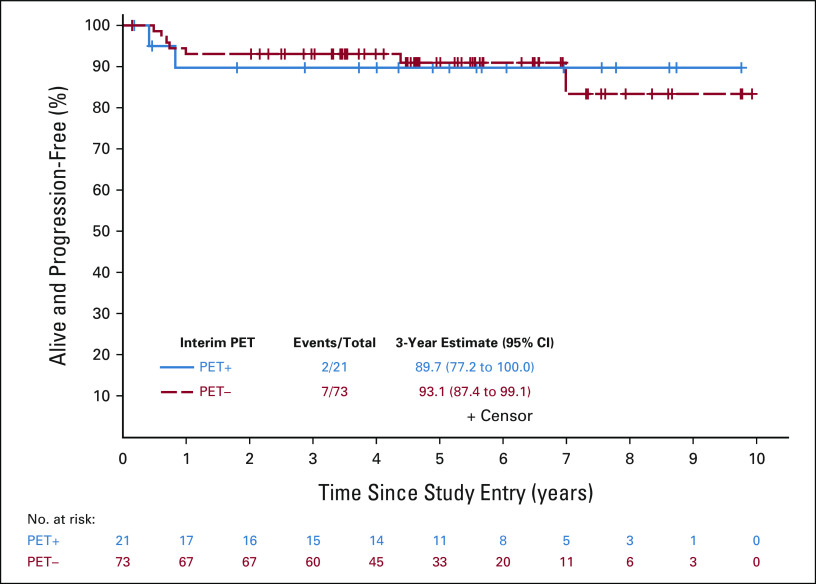
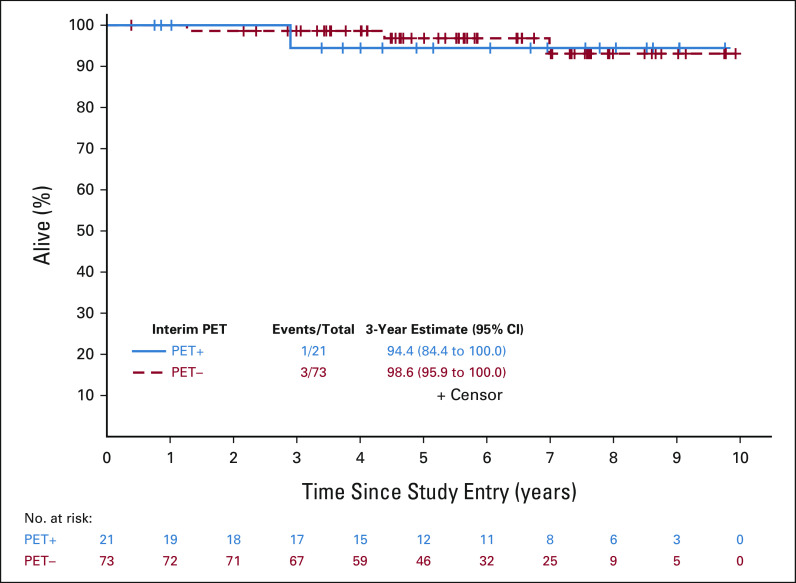
Results: Of 94 evaluable patients, 53% were female with median age 30 years (range, 18-58 years). Eight-five (90%) had stage II disease, including 48 (51%) with stage IIB/IIBE. Seventy-eight (78%) were PET2- and 21 (22%) were PET2+. The predominant toxicity was neutropenia, with 9% of patients developing febrile neutropenia and one developing sepsis. The primary end point of 3-year progression-free survival (PFS) was 93.1% in PET2- and 89.7% in PET2+ patients. Three-year overall survival was 98.6% and 94.4%, respectively. The estimated hazard ratio comparing PFS of patients with PET2+ and patients with PET2- was 1.03 (85% upper bound 2.38) and was significantly less than the null hypothesis of 4.1 (one-sided P = .04).
Conclusion: Our study of PET-adapted therapy in bulky stage I/II cHL met its primary goal and was associated with an excellent 3-year PFS rate of 92.3% in all patients, with the majority being spared radiotherapy and exposure to intensified chemotherapy.
Trial registration: ClinicalTrials.gov NCT01118026.
Conflict of interest statement
Positron Emission Tomography–Adapted Therapy in Bulky Stage I/II Classic Hodgkin Lymphoma: CALGB 50801 (Alliance)
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
Figures
References
-
- Colonna P, Jais JP, Desablens B, et al. Mediastinal tumor size and response to chemotherapy are the only prognostic factors in supradiaphragmatic Hodgkin's disease treated by ABVD plus radiotherapy: Ten-year results of the Paris-Ouest-France 81/12 trial, including 262 patients. J Clin Oncol. 1996;14:1928–1935. - PubMed
-
- Advani RH, Hong F, Fisher RI, et al. Randomized phase III trial comparing ABVD plus radiotherapy with the Stanford V regimen in patients with stages I or II locally extensive, bulky mediastinal Hodgkin lymphoma: A subset analysis of the North American Intergroup E2496 trial. J Clin Oncol. 2015;33:1936–1942. - PMC - PubMed
-
- Hancock SL, Tucker MA, Hoppe RT. Breast cancer after treatment of Hodgkin's disease. J Natl Cancer Inst. 1993;85:25–31. - PubMed
-
- Ng AK, Bernardo MV, Weller E, et al. Second malignancy after Hodgkin disease treated with radiation therapy with or without chemotherapy: Long-term risks and risk factors. Blood. 2002;100:1989–1996. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
