

Clinical effectiveness and safety of spinal anaesthesia compared with general anaesthesia in patients undergoing hip fracture surgery using a consensus-based core outcome set and patient-and public-informed outcomes: a systematic review and meta-analysis of randomised controlled trials
- PMID: 36270701
- PMCID: PMC9642835
- DOI: 10.1016/j.bja.2022.07.031
Clinical effectiveness and safety of spinal anaesthesia compared with general anaesthesia in patients undergoing hip fracture surgery using a consensus-based core outcome set and patient-and public-informed outcomes: a systematic review and meta-analysis of randomised controlled trials
Abstract
Background: We conducted a systematic review and meta-analysis of contemporary RCTs to determine the clinical effectiveness of spinal vs general anaesthesia (SA vs GA) in patients undergoing hip fracture surgery using a consensus-based core outcome set, and outcomes defined as important by patient and public involvement (PPI) initiatives.
Methods: RCTs comparing any of the core outcomes (mortality, time from injury to surgery, acute coronary syndrome, hypotension, acute kidney injury, delirium, pneumonia, orthogeriatric input, being out of bed at day 1 postoperatively, and pain) or PPI-defined outcomes (return to preoperative residence, quality of life, and mobility status) between SA and GA were identified from MEDLINE, Embase, Cochrane Library, and Web of Science (2000 to February 2022). Pooled relative risks (RRs) and mean differences (95% confidence intervals [CIs]) were estimated.
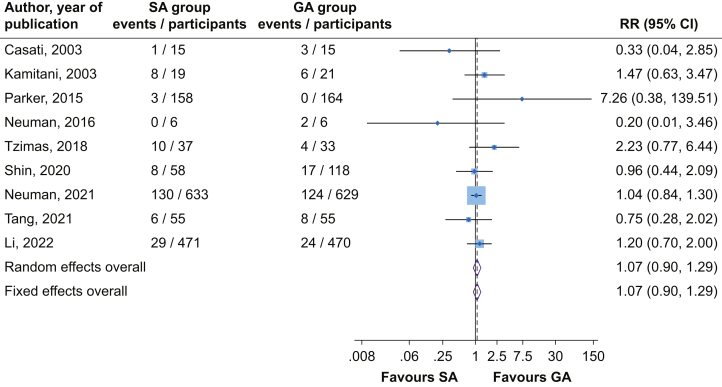
Results: There was no significant difference in the risk of delirium comparing SA vs GA (RR=1.07; 95% CI, 0.90-1.29). Comparing SA vs GA, the RR for mortality was 0.56 (95% CI, 0.22-1.44) in-hospital, 1.07 (95% CI, 0.52-2.23) at 30 days, and 1.08 (95% CI, 0.55-2.12) at 90 days. Spinal anaesthesia reduced the risk of acute kidney injury compared with GA: RR=0.59 (95% CI, 0.39-0.89). There were no significant differences in the risk of other outcomes. Few studies reported PPI-defined outcomes, with most studies reporting on one to three core outcomes.
Conclusions: Except for acute kidney injury, there were no differences between SA and GA in hip fracture surgery when using a consensus-based core outcome set and patient and public involvement-defined outcomes. Most studies reported limited outcomes from the core outcome set, and few reported outcomes important to patients, which should be considered when designing future RCTs.
Prospero registration: CRD42021275206.
Keywords: complication; core outcome set; general anaesthesia; hip fracture; meta-analysis; mortality; spinal anaesthesia; systematic review.
Copyright © 2022 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures




Comment in
-
There is (probably) no (meaningful) difference in (most) outcomes between 'spinal' and 'general' anaesthesia for hip fracture surgery: time to move forward.Br J Anaesth. 2023 Apr;130(4):385-389. doi: 10.1016/j.bja.2023.01.013. Epub 2023 Feb 16. Br J Anaesth. 2023. PMID: 36801101
References
-
- Cooper C., Campion G., Melton L.J., 3rd Hip fractures in the elderly: a world-wide projection. Osteoporos Int. 1992;2:285–289. - PubMed
-
- Johnell O., Kanis J. An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporos Int. 2004;15:897–902. - PubMed
-
- Johnell O., Kanis J. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17:1726–1733. - PubMed
-
- National hip fracture database (NHFD) Royal College of Physicians; London: 2017. Annual report 2017.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
