

Neoadjuvant durvalumab for resectable non-small-cell lung cancer (NSCLC): results from a multicenter study (IFCT-1601 IONESCO)
- PMID: 36270733
- PMCID: PMC9594538
- DOI: 10.1136/jitc-2022-005636
Neoadjuvant durvalumab for resectable non-small-cell lung cancer (NSCLC): results from a multicenter study (IFCT-1601 IONESCO)
Abstract
Background: The IONESCO (IFCT-1601) trial assessed the feasibility of neoadjuvant durvalumab, for early-stage resectable non-small-cell lung cancer (NSCLC).
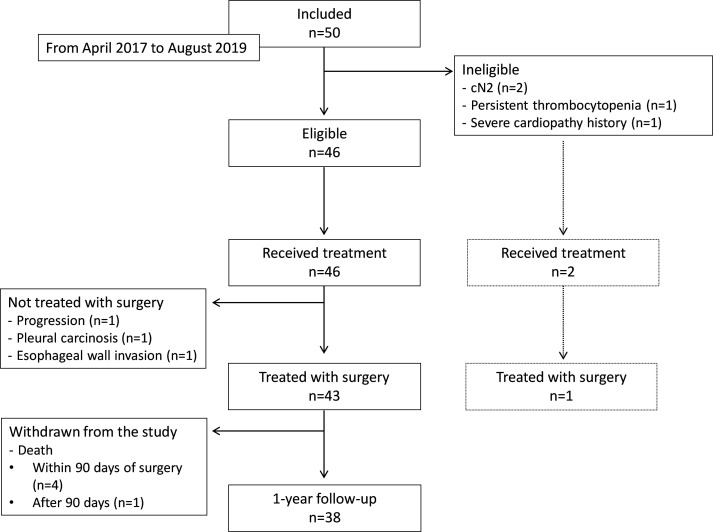
Methods: In a multicenter, single-arm, phase II trial, patients with IB (≥4 cm)-IIIA, non-N2, resectable NSCLC received three doses of durvalumab (750 mg every 2 weeks) and underwent surgery between 2 and 14 days after the last infusion. The primary endpoint was the complete surgical resection rate. Secondary endpoints included tumor response rate, major histopathological response (MPR: ≤10% remaining viable tumor cells), disease-free survival (DFS), overall survival (OS), durvalumab-related safety, and 90-day postoperative mortality (NCT03030131).
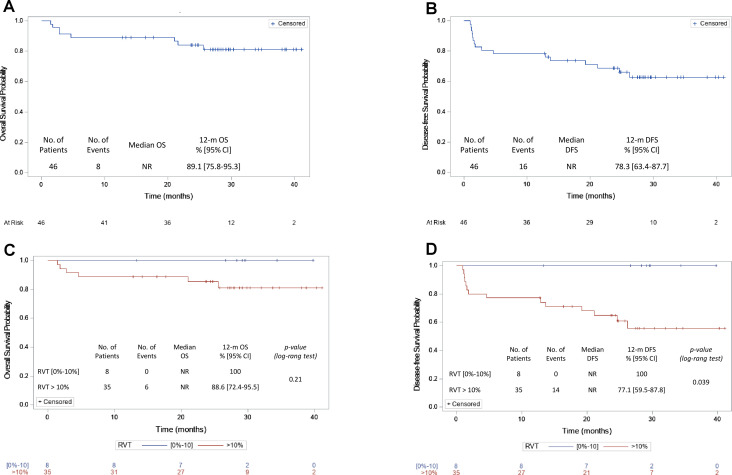
Results: Forty-six patients were eligible (median age 60.9 years); 67% were male, 98% were smokers, and 41% had squamous cell carcinoma. Regarding tumor response, 9% had a partial response, 78% had stable disease, and 13% had progressive disease. Among the operated patients (n=43), 41 achieved complete resection (89%, 95% CI 80.1% to 98.1%)), and eight achieved MPR (19%). The 12-month median OS and DFS rates were 89% (95% CI 75.8% to 95.3%) and 78% (95% CI 63.4% to 87.7%), respectively (n=46). The median follow-up was 28.4 months (12.8-41.1). All patients in whom MPR was achieved were disease-free at 12 months compared to only 11% of those with >10% residual tumor cells (p=0.04). No durvalumab-related serious or grade 3-5 events were reported. The unexpected 90-day postoperative mortality of four patients led to premature study termination. None of these four deaths was considered secondary to direct durvalumab-related toxicity.
Conclusions: Neoadjuvant durvalumab given as monotherapy was associated with an 89% complete resection rate and an MPR of 19%. Despite an unexpectedly high rate of postoperative deaths, which prevented us from completing the trial, we were able to show a significant association between MPR and DFS.
Keywords: Biomarkers, Tumor; Immunotherapy; Lung Neoplasms; Programmed Cell Death 1 Receptor.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: Marie Wislez, reports grants from Astra-Zeneca, honoraria for speaker’s bureau from Roche, Bristol Myers Squibb and Boehringer Ingelheim, participation on a Data Safety Monitoring Board or Advisory Board from Astra-Zeneca, Merck Sharp and Dohme and Novartis, non-financial interests from Astra-Zeneca, Bristol Myers Squibb, Merck Sharp and Dohme, Novartis, Lilly Merck KgA, Merus, GlaxoSmithKline and Amgen, outside the submitted work. Julien Mazières reports honoraria for lectures from Bristol Myers Squibb, Roche Genentech, Astra-Zeneca and Merck Sharp and Dohme, outside the submitted work. Gérard Zalcman reports grants from Roche and Bristol Myers Squibb, payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Astra-Zeneca and Bristol Myers Squibb, support for attending meetings and/or travel from Astra-Zeneca, Abbvie, Bristol Myers Squibb and Pfizer, participation on a Data Safety Monitoring Board or Advisory Board from Astra-Zeneca, Inventiva, Da Volterra and Bristol Myers Squibb, outside the submitted work. Olivier Molinier reports participation on a Data Safety Monitoring Board or Advisory Board from Astra-Zeneca, outside the submitted work. Virginie Westeel reports payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Astra-Zeneca, Bristol Myers Squibb, Merck Sharp and Dohme and Roche, Support for attending meetings and/or travel from Astra-Zeneca, Bristol Myers Squibb, Merck Sharp and Dohme, Pfizer and Roche, Participation on a Data Safety Monitoring Board or Advisory Board from Astra-Zeneca, Bristol Myers Squibb, Merck Sharp and Dohme, Takeda and Roche, outside the submitted work. All other authors have nothing to disclose.
Figures
References
-
- Wakelee HA, Altorki NK, Zhou C, et al. . IMpower010: primary results of a phase III global study of atezolizumab versus best supportive care after adjuvant chemotherapy in resected stage IB-IIIA non-small cell lung cancer (NSCLC). JCO 2021;39:8500. 10.1200/JCO.2021.39.15_suppl.8500 - DOI
-
- Paz-Ares L, O'Brien MER, Mauer M, et al. . VP3-2022: pembrolizumab (pembro) versus placebo for early-stage non-small cell lung cancer (NSCLC) following complete resection and adjuvant chemotherapy (chemo) when indicated: randomized, triple-blind, phase III EORTC-1416-LCG/ETOP 8-15 – PEARLS/KEYNOTE-091 study. Annals of Oncology 2022;33:451–3. 10.1016/j.annonc.2022.02.224 - DOI
-
- Liu J, Blake SJ, Yong MCR, et al. . Improved efficacy of neoadjuvant compared to adjuvant immunotherapy to eradicate metastatic disease. Cancer Discov 2016;6:1382–99. 10.1158/2159-8290.CD-16-0577 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous