Randomized Double-Blind Placebo-Controlled Trial of the Corticosteroid-Sparing Effects of Immunoglobulin in Myasthenia Gravis
- PMID: 36270895
- PMCID: PMC9969924
- DOI: 10.1212/WNL.0000000000201501
Randomized Double-Blind Placebo-Controlled Trial of the Corticosteroid-Sparing Effects of Immunoglobulin in Myasthenia Gravis
Erratum in
-
Randomized Double-Blind Placebo-Controlled Trial of the Corticosteroid-Sparing Effects of Immunoglobulin in Myasthenia Gravis.Neurology. 2023 Sep 12;101(11):501. doi: 10.1212/WNL.0000000000207433. Epub 2023 Apr 25. Neurology. 2023. PMID: 37185127 Free PMC article. No abstract available.
-
Corrections to Null Hypothesis Articles.Neurology. 2025 May 13;104(9):e213475. doi: 10.1212/WNL.0000000000213475. Epub 2025 Apr 4. Neurology. 2025. PMID: 40184595 Free PMC article. No abstract available.
Abstract
Background and objectives: Myasthenia gravis (MG) is an autoimmune disease characterized by dysfunction at the neuromuscular junction. Treatment frequently includes corticosteroids (CSs) and IV immunoglobulin (IVIG). This study was conducted to determine whether immune globulin (human), 10% caprylate/chromatography purified (IGIV-C) could facilitate CS dose reduction in CS-dependent patients with MG.
Methods: In this randomized double-blind placebo-controlled trial, CS-dependent patients with MG (Myasthenia Gravis Foundation of America Class II-Iva; AChR+) received a loading dose of 2 g/kg IGIV-C over 2 days (maximum 80 g/d) or placebo at week 0 (baseline). Maintenance doses (1 g/kg IGIV-C or placebo) were administered every 3 weeks through week 36. Tapering of CS was initiated at week 9 and continued through week 36 unless the patient worsened (quantitative MG score ≥4 points from baseline). CS doses were increased (based on the current CS dose) in patients who worsened. Patients were withdrawn if worsening failed to improve within 6 weeks or if a second CS increase was required. The primary efficacy end point (at week 39) was a ≥50% reduction in CS dose. Secondary and safety end points were assessed throughout the study and follow-up (weeks 42 and 45). The study results and full protocol are available at clinicaltrials.gov/ct2/show/NCT02473965.
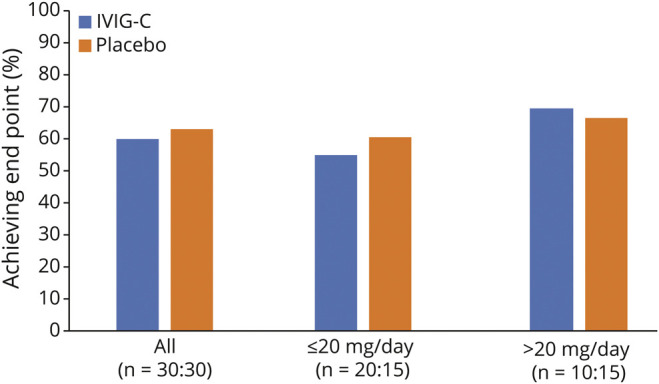
Results: The primary end point (≥50% reduction in CS dose) showed no significant difference between the IGIV-C treatment (60.0% of patients) and placebo (63.3%). There were no significant differences for secondary end points. Safety data indicated that IGIV-C was well tolerated.
Discussion: In this study, IGIV-C was not more effective than placebo in reducing daily CS dose. These results suggest that the effects of IGIV-C and CS are not synergistic and may be mechanistically different.
Trial registration information: The trial was registered on clinicaltrialsregister.eu (EudraCT #: 2013-005099-17) and clinicaltrials.gov (identifier NCT02473965).
Classification of evidence: This study provides Class II evidence that IVIG infusions in adult patients with MG do not increase the percentage of patients achieving a ≥50% reduction in corticosteroid dose compared with placebo.
© 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures