

Oxygen targets and 6-month outcome after out of hospital cardiac arrest: a pre-planned sub-analysis of the targeted hypothermia versus targeted normothermia after Out-of-Hospital Cardiac Arrest (TTM2) trial
- PMID: 36271410
- PMCID: PMC9585831
- DOI: 10.1186/s13054-022-04186-8
Oxygen targets and 6-month outcome after out of hospital cardiac arrest: a pre-planned sub-analysis of the targeted hypothermia versus targeted normothermia after Out-of-Hospital Cardiac Arrest (TTM2) trial
Abstract
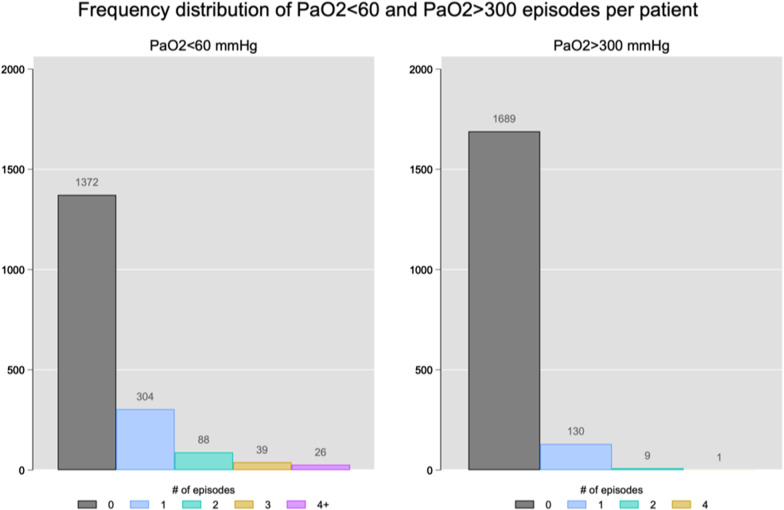
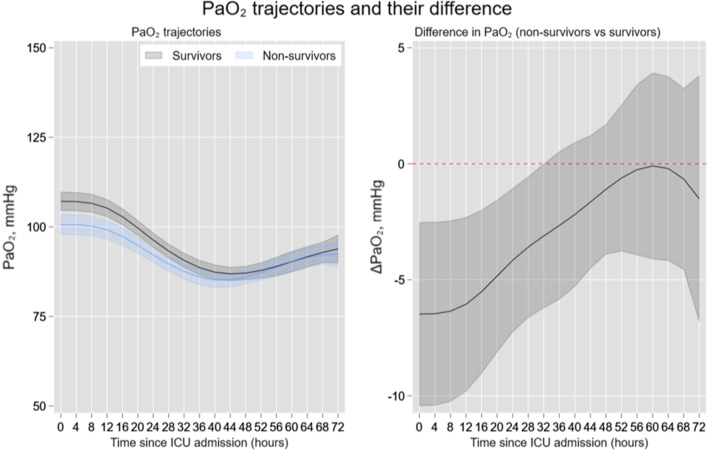
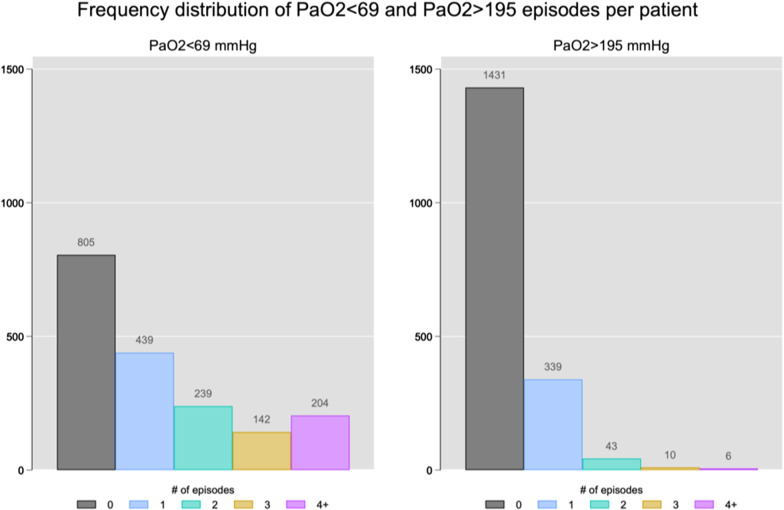
Background: Optimal oxygen targets in patients resuscitated after cardiac arrest are uncertain. The primary aim of this study was to describe the values of partial pressure of oxygen values (PaO2) and the episodes of hypoxemia and hyperoxemia occurring within the first 72 h of mechanical ventilation in out of hospital cardiac arrest (OHCA) patients. The secondary aim was to evaluate the association of PaO2 with patients' outcome.
Methods: Preplanned secondary analysis of the targeted hypothermia versus targeted normothermia after OHCA (TTM2) trial. Arterial blood gases values were collected from randomization every 4 h for the first 32 h, and then, every 8 h until day 3. Hypoxemia was defined as PaO2 < 60 mmHg and severe hyperoxemia as PaO2 > 300 mmHg. Mortality and poor neurological outcome (defined according to modified Rankin scale) were collected at 6 months.
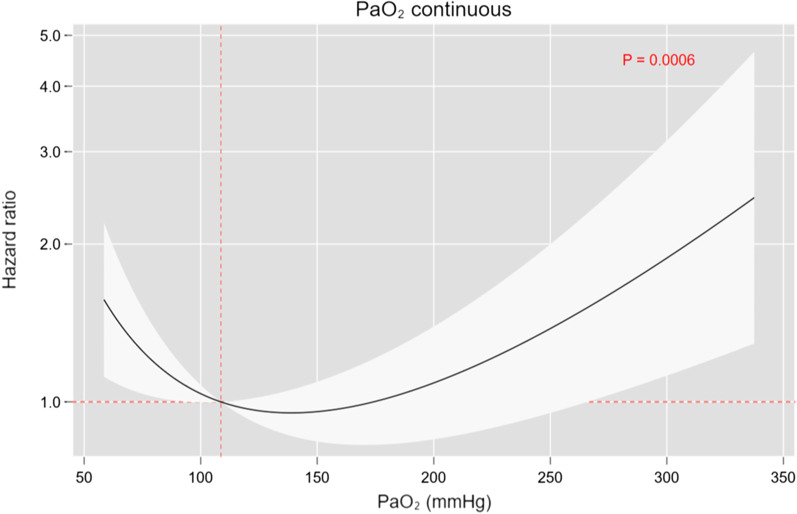
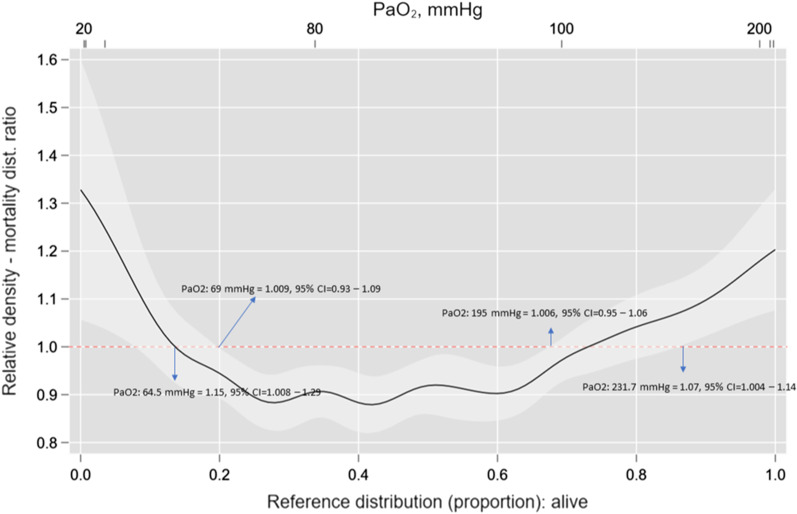
Results: 1418 patients were included in the analysis. The mean age was 64 ± 14 years, and 292 patients (20.6%) were female. 24.9% of patients had at least one episode of hypoxemia, and 7.6% of patients had at least one episode of severe hyperoxemia. Both hypoxemia and hyperoxemia were independently associated with 6-month mortality, but not with poor neurological outcome. The best cutoff point associated with 6-month mortality for hypoxemia was 69 mmHg (Risk Ratio, RR = 1.009, 95% CI 0.93-1.09), and for hyperoxemia was 195 mmHg (RR = 1.006, 95% CI 0.95-1.06). The time exposure, i.e., the area under the curve (PaO2-AUC), for hyperoxemia was significantly associated with mortality (p = 0.003).
Conclusions: In OHCA patients, both hypoxemia and hyperoxemia are associated with 6-months mortality, with an effect mediated by the timing exposure to high values of oxygen. Precise titration of oxygen levels should be considered in this group of patients.
Trial registration: clinicaltrials.gov NCT02908308 , Registered September 20, 2016.
Keywords: Cardiac arrest; Hyperoxemia; Hypoxemia; Mortality; Neurological outcome.
© 2022. The Author(s).
Conflict of interest statement
Dr. Saxena is receiving consulting fees from Bard Medical; Dr. Young is receiving lecture fees from Bard Medical; Dr. Taccone is receiving grant support from Bard Medical and ZOLL Medical; Dr. Nichol is receiving grant support, paid to University College Dublin, from AM Pharma and grant sup-port, paid to Monash University, from Baxter Healthcare; Dr. Chew is receiving lecture fees from Edwards Lifesciences; Dr. Friberg is receiving fees for academic advising from TEQCool; and Dr. Nielsen is receiving lecture fees from Bard Medical and consulting fees from BrainCool. Dr Badenes is supported by INCLIVA. Dr Robba received fees for lectures from Masimo, and GE. Dr. Battaglini received fees for lectures from Baxter. No other potential conflict of interest relevant to this article was reported.
Figures
References
-
- Sasson C, Rogers MAM, Dahl J, Kellermann AL. Predictors of survival from out-of-hospital cardiac arrest. Circ Cardiovasc Qual Outcomes. 2010;3:63–81. - PubMed
-
- Zandbergen EGJ, de Haan RJ, Reitsma JB, Hijdra A. Survival and recovery of consciousness in anoxic-ischemic coma after cardiopulmonary resuscitation. Intensive Care Med. 2003;29:1911–1915. - PubMed
-
- Eastwood GM, Tanaka A, Espinoza EDV, Peck L, Young H, Mårtensson J, et al. Conservative oxygen therapy in mechanically ventilated patients following cardiac arrest: a retrospective nested cohort study. Resuscitation. 2016;101:108–114. - PubMed
-
- Nolan JP, Neumar RW, Adrie C, Aibiki M, Berg RA, Böttiger BW, et al. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. Resuscitation. 2008;79:350–379. - PubMed
