

Dehydration is associated with production of organic osmolytes and predicts physical long-term symptoms after COVID-19: a multicenter cohort study
- PMID: 36271419
- PMCID: PMC9585783
- DOI: 10.1186/s13054-022-04203-w
Dehydration is associated with production of organic osmolytes and predicts physical long-term symptoms after COVID-19: a multicenter cohort study
Abstract
Background: We have previously shown that iatrogenic dehydration is associated with a shift to organic osmolyte production in the general ICU population. The aim of the present investigation was to determine the validity of the physiological response to dehydration known as aestivation and its relevance for long-term disease outcome in COVID-19.
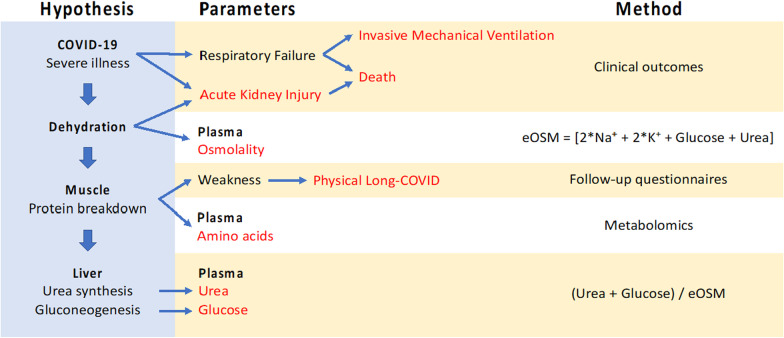
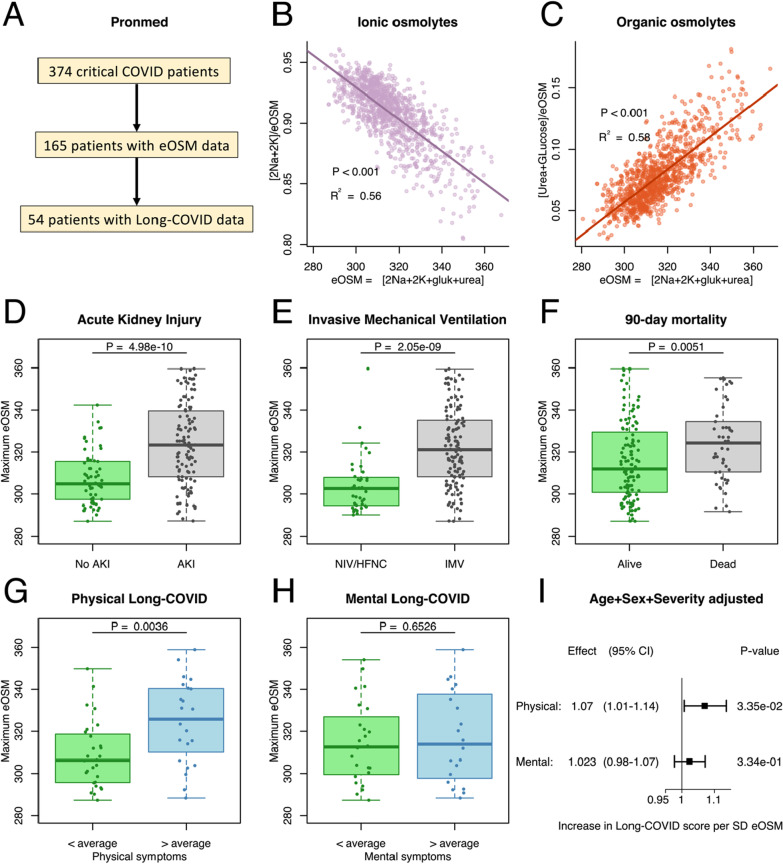
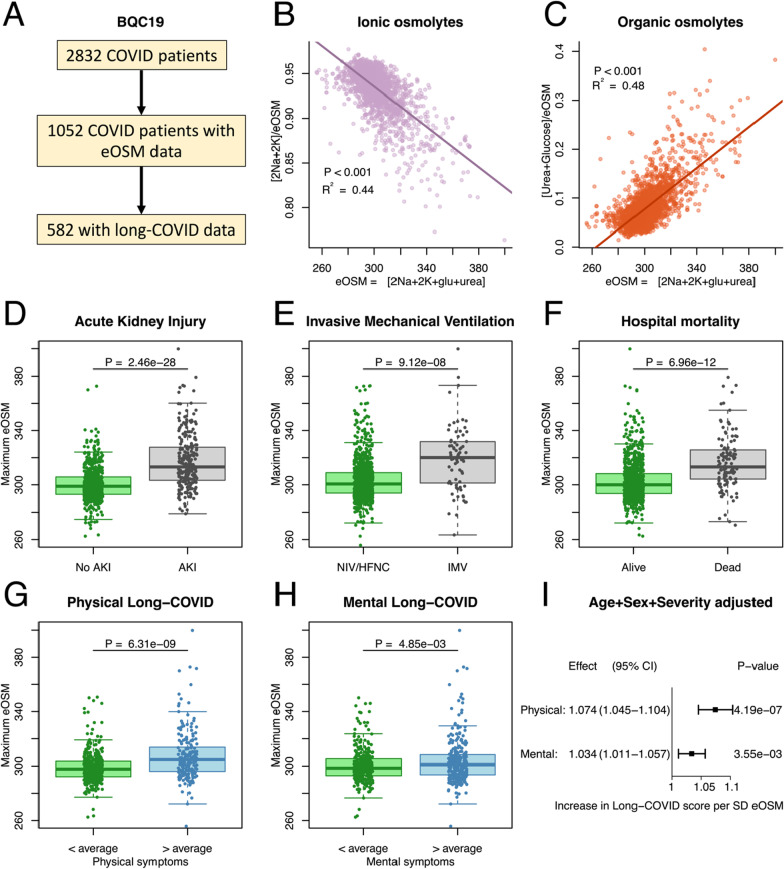
Methods: The study includes 374 COVID-19 patients from the Pronmed cohort admitted to the ICU at Uppsala University Hospital. Dehydration data was available for 165 of these patients and used for the primary analysis. Validation was performed in Biobanque Québécoise de la COVID-19 (BQC19) using 1052 patients with dehydration data. Dehydration was assessed through estimated osmolality (eOSM = 2Na + 2 K + glucose + urea), and correlated to important endpoints including death, invasive mechanical ventilation, acute kidney injury, and long COVID-19 symptom score grouped by physical or mental.
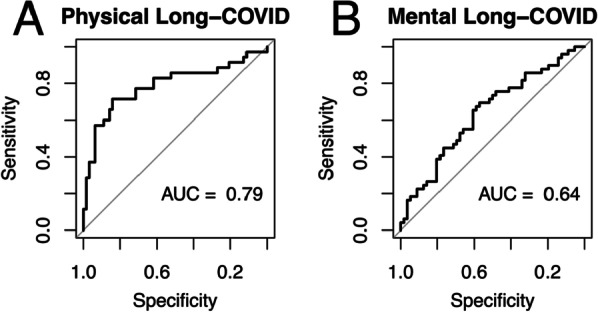
Results: Increasing eOSM was correlated with increasing role of organic osmolytes for eOSM, while the proportion of sodium and potassium of eOSM were inversely correlated to eOSM. Acute outcomes were associated with pronounced dehydration, and physical long-COVID was more strongly associated with dehydration than mental long-COVID after adjustment for age, sex, and disease severity. Metabolomic analysis showed enrichment of amino acids among metabolites that showed an aestivating pattern.
Conclusions: Dehydration during acute COVID-19 infection causes an aestivation response that is associated with protein degradation and physical long-COVID.
Trial registration: The study was registered à priori (clinicaltrials.gov: NCT04316884 registered on 2020-03-13 and NCT04474249 registered on 2020-06-29).
Keywords: Acute kidney injury; Aestivation; Intensive care medicine; Long-COVID; SARS-CoV-2; Urea synthesis.
© 2022. The Author(s).
Conflict of interest statement
JBR served as an advisor to GlaxoSmithKline and Deerfield Capital, and is the founder and CEO of 5 Prime Sciences. VF and YF are employed by 5 Prime Sciences. YF consults for Fulcrum Genomics. The other authors declare that they have no conflicts of interest.
Figures
References
-
- Nihlen S, Frithiof R, Titze J, Kawati R, Rasmusson J, Rylander C, Pikwer A, Castegren M, Belin A, Hultstrom M, et al. The contribution of plasma urea to total osmolality during iatrogenic fluid reduction in critically ill patients. Function (Oxf) 2022;3(1):zqab055. doi: 10.1093/function/zqab055. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
