

Association of the gallbladder or biliary diseases with dipeptidyl peptidase 4 inhibitors in patients with type 2 diabetes: a meta-analysis of randomized controlled trials
- PMID: 36271423
- PMCID: PMC9585736
- DOI: 10.1186/s13098-022-00924-8
Association of the gallbladder or biliary diseases with dipeptidyl peptidase 4 inhibitors in patients with type 2 diabetes: a meta-analysis of randomized controlled trials
Abstract
Background: Previous studies have shown inconsistent conclusions regarding the association between incretin-based therapies and the risk of developing gallbladder or biliary diseases. We conducted a meta-analysis to evaluate the risk of gallbladder or biliary diseases associated with dipeptidyl peptidase 4 inhibitors (DPP4i) in patients with type 2 diabetes.
Methods: The PubMed, Embase, Cochrane Library, and ClinicalTrials.gov databases were searched (from inception up to March 14, 2022) for published randomized controlled trials (RCTs) that compared DPP4i with placebo or other glucose-lowering drugs in patients with type 2 diabetes. The outcomes of interest were cholecystitis, cholangitis, cholelithiasis, bile duct stones, and biliary colic. Relative risks (RRs) and 95% confidence intervals (CI) were pooled using a random-effects model. Subgroup analyses were performed according to patient age, trial duration, and types of DPP4i.
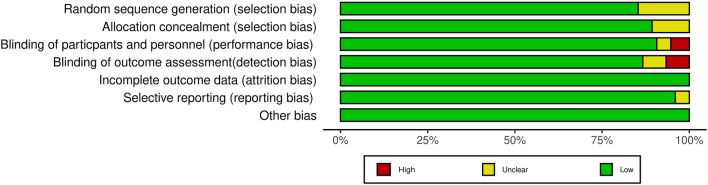
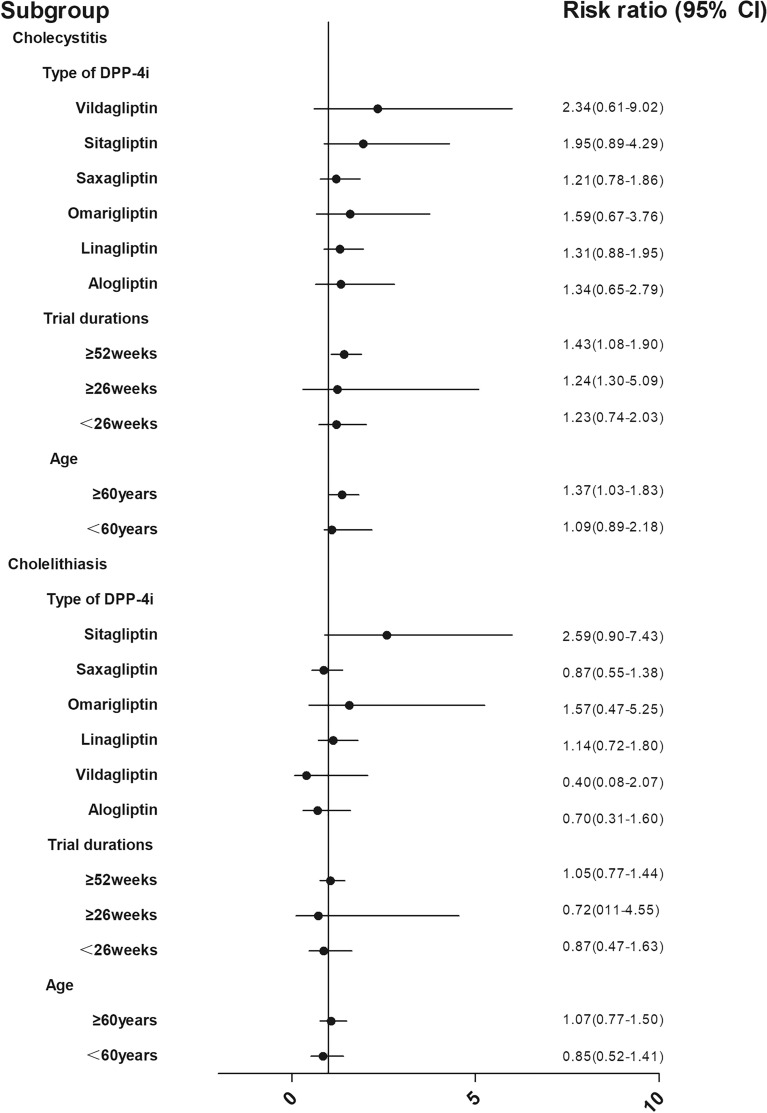
Results: In total, 97,150 participants from 75 eligible RCTs were included in the meta-analysis. DPP4i were associated with an increased risk of composite of gallbladder or biliary diseases (RR 1.20 [95% CI 1.01-1.42]) and cholecystitis (RR 1.38 [95% CI 1.08-1.75]). Among all included trials, DPP4i showed no association with the following manifestations of gallbladder or biliary diseases: cholelithiasis (RR 1.00 [95% CI 0.76-1.32]), cholangitis (RR 0.81 [95% CI 0.39-1.66]), bile duct stones (RR 1.08 [95% CI 0.57-2.05]), and biliary colic (RR 0.72 [95% CI 0.23-2.25]). Subgroup analyses showed that DPP4i were associated with a higher risk of cholecystitis in older patients (RR 1.37 [95% CI 1.03-1.83]) compared with younger patients (RR 1.08 [95% CI 0.89-2.18]) and in those with a longer duration of drug use (RR 1.43 [95% CI 1.08-1.89]) compared with shorter use (RR 1.23 [95% CI 0.74-2.03]).
Conclusions: This systematic review and meta-analysis of RCTs found that the use of DPP4i was associated with an increased risk of cholecystitis, especially in patients of advanced age or in those who were exposed to the drugs for a long period of time.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



Similar articles
-
Incretin-based drugs and the risk of gallbladder or biliary tract diseases among patients with type 2 diabetes across categories of body mass index: a nationwide cohort study.Lancet Reg Health West Pac. 2025 Mar 10;56:101242. doi: 10.1016/j.lanwpc.2024.101242. eCollection 2025 Mar. Lancet Reg Health West Pac. 2025. PMID: 40226782 Free PMC article.
-
Association of Glucagon-Like Peptide-1 Receptor Agonist Use With Risk of Gallbladder and Biliary Diseases: A Systematic Review and Meta-analysis of Randomized Clinical Trials.JAMA Intern Med. 2022 May 1;182(5):513-519. doi: 10.1001/jamainternmed.2022.0338. JAMA Intern Med. 2022. PMID: 35344001 Free PMC article.
-
Safety issues of tirzepatide (pancreatitis and gallbladder or biliary disease) in type 2 diabetes and obesity: a systematic review and meta-analysis.Front Endocrinol (Lausanne). 2023 Oct 16;14:1214334. doi: 10.3389/fendo.2023.1214334. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37908750 Free PMC article.
-
Dipeptidyl peptidase-4 inhibitors and cancer risk in patients with type 2 diabetes: a meta-analysis of randomized clinical trials.Sci Rep. 2017 Aug 15;7(1):8273. doi: 10.1038/s41598-017-07921-2. Sci Rep. 2017. PMID: 28811622 Free PMC article.
-
Preoperative versus intraoperative endoscopic sphincterotomy in patients with gallbladder and suspected common bile duct stones: system review and meta-analysis.Surg Endosc. 2013 Jul;27(7):2454-65. doi: 10.1007/s00464-012-2757-7. Epub 2013 Jan 26. Surg Endosc. 2013. PMID: 23355158 Review.
Cited by
-
Association between GLP-1 RAs and DPP-4 inhibitors with biliary disorders: pharmacovigilance analysis.Front Pharmacol. 2025 Feb 17;16:1509561. doi: 10.3389/fphar.2025.1509561. eCollection 2025. Front Pharmacol. 2025. PMID: 40041492 Free PMC article.
-
Incretin-based drugs and the risk of gallbladder or biliary tract diseases among patients with type 2 diabetes across categories of body mass index: a nationwide cohort study.Lancet Reg Health West Pac. 2025 Mar 10;56:101242. doi: 10.1016/j.lanwpc.2024.101242. eCollection 2025 Mar. Lancet Reg Health West Pac. 2025. PMID: 40226782 Free PMC article.
-
Association between incretin-based drugs and risk of cholangiocarcinoma among patients with type 2 diabetes: A large population-based matched cohort study.J Clin Transl Endocrinol. 2024 Sep 18;38:100370. doi: 10.1016/j.jcte.2024.100370. eCollection 2024 Dec. J Clin Transl Endocrinol. 2024. PMID: 39386155 Free PMC article.
References
-
- Nauck MA, Muus Ghorbani ML, Kreiner E, et al. Effects of liraglutide compared with placebo on events of acute gallbladder or biliary disease in patients with type 2 diabetes at high risk for cardiovascular events in the LEADER randomized trial. Diabetes Care. 2019;42(10):1912–1920. doi: 10.2337/dc19-0415. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
