

Viral Shedding 1 Year Following First-Episode Genital HSV-1 Infection
- PMID: 36272098
- PMCID: PMC9588168
- DOI: 10.1001/jama.2022.19061
Viral Shedding 1 Year Following First-Episode Genital HSV-1 Infection
Abstract
Importance: Herpes simplex virus type 1 (HSV-1) is the leading cause of first-episode genital herpes in many countries.
Objective: To inform counseling messages regarding genital HSV-1 transmission, oral and genital viral shedding patterns among persons with first-episode genital HSV-1 infection were assessed. The trajectory of the development of HSV-specific antibody and T-cell responses was also characterized.
Design, setting, and participants: Prospective cohort followed up for up to 2 years, with 82 participants followed up between 2013 and 2018. Participants were recruited from sexual health and primary care clinics in Seattle, Washington. Persons with laboratory-documented first-episode genital HSV-1 infection, without HIV infection or current pregnancy, were referred for enrollment.
Exposures: First-episode genital HSV-1 infection.
Main outcomes and measures: Genital and oral HSV-1 shedding and lesion rates at 2 months, 11 months, and up to 2 years after initial genital HSV-1 infection. Participants self-collected oral and genital swabs for HSV polymerase chain reaction testing for 30 days at 2 and 11 months and up to 2 years after diagnosis of genital HSV-1. Blood samples were collected at serial time points to assess immune responses to HSV-1. Primary HSV-1 infection was defined as absent HSV antibody at baseline or evolving antibody profile using the University of Washington HSV Western Blot. HSV-specific T-cell responses were detected using interferon γ enzyme-linked immunospot.
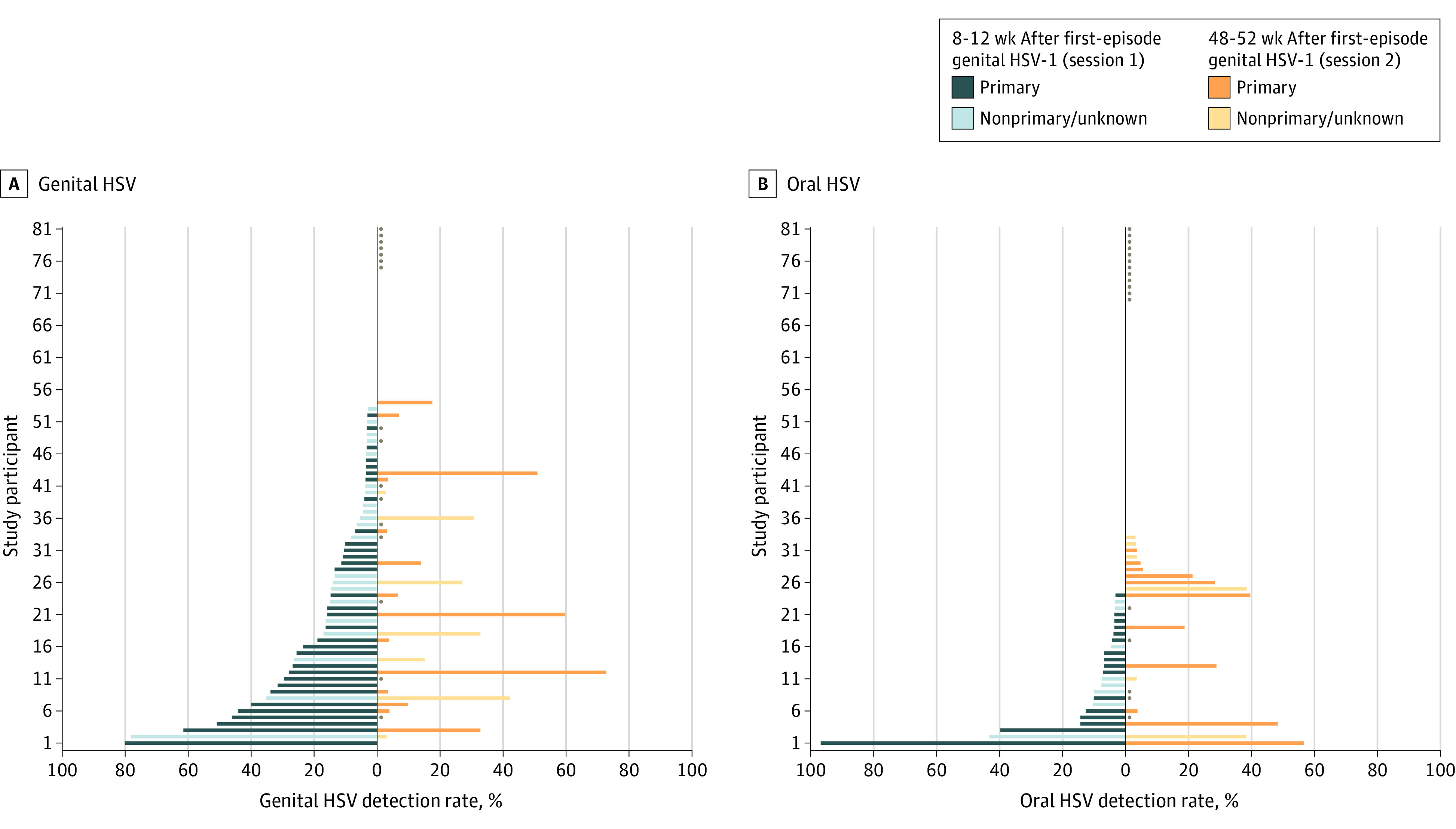
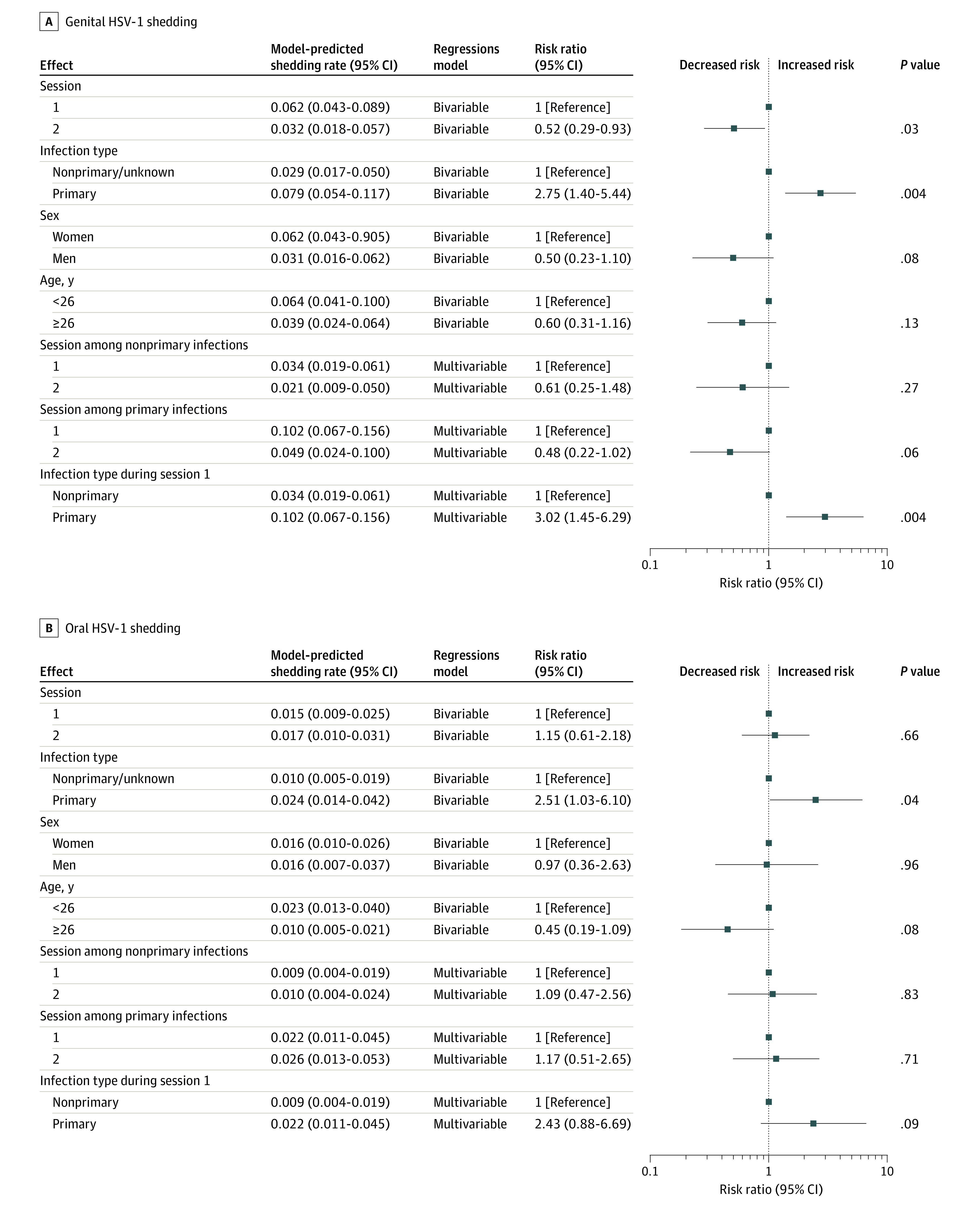
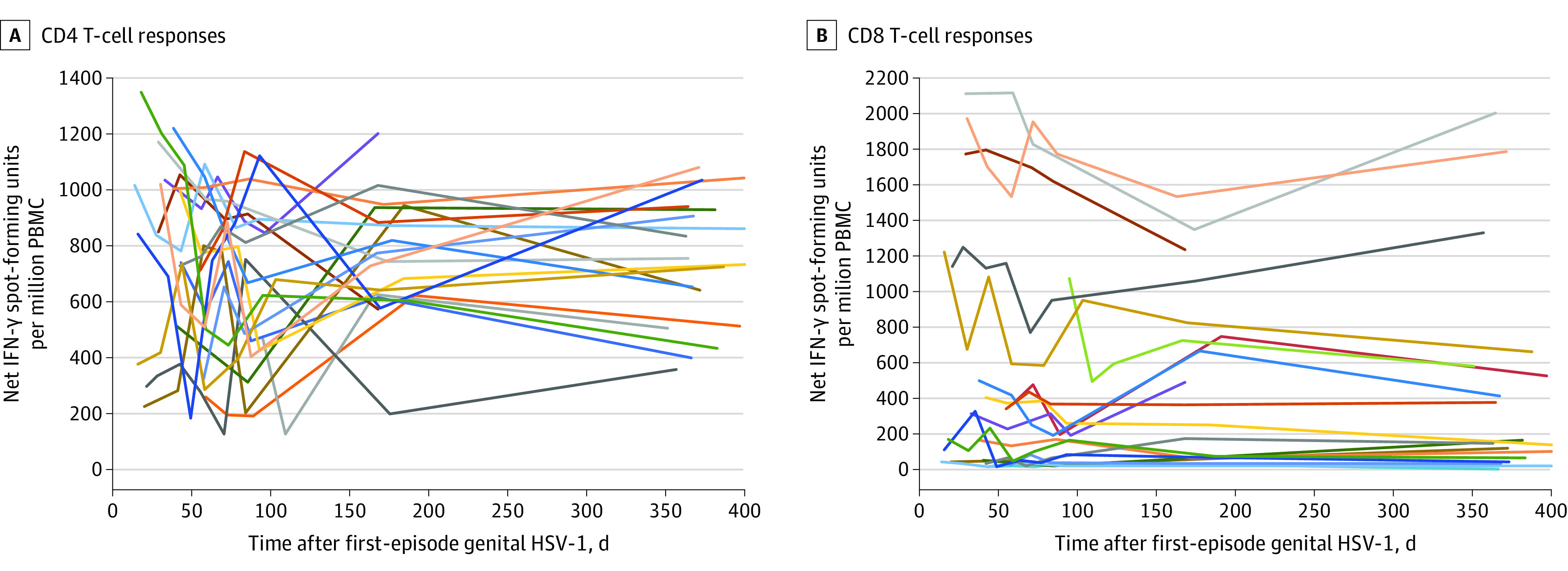
Results: Among the 82 participants, the median (range) age was 26 (16-64) years, 54 (65.9%) were women, and 42 (51.2%) had primary HSV-1 infection. At 2 months, HSV-1 was detected from the genital tract in 53 participants (64.6%) and in the mouth in 24 participants (29.3%). Genital HSV-1 shedding was detected on 275 of 2264 days (12.1%) at 2 months and declined significantly to 122 of 1719 days (7.1%) at 11 months (model-predicted rate, 6.2% [95% CI, 4.3%-8.9%] at 2 months vs 3.2% [95% CI, 1.8%-5.7%] at 11 months; relative risk, 0.52 [95% CI, 0.29-0.93]). Genital lesions were rare, reported on 65 of 2497 days (2.6%) at 2 months and 72 of 1872 days (3.8%) at 11 months. Oral HSV-1 shedding was detected on 88 of 2247 days (3.9%) at 2 months. Persons with primary HSV-1 infection had a higher risk of genital shedding compared with those with nonprimary infection (model-predicted rate, 7.9% [95% CI, 5.4%-11.7%] vs 2.9% [95% CI, 1.7%-5.0%]; relative risk, 2.75 [95% CI, 1.40-5.44]). Polyfunctional HSV-specific CD4+ and CD8+ T-cell responses were maintained during the follow-up period.
Conclusions and relevance: Genital HSV-1 shedding was frequent after first-episode genital HSV-1, particularly among those with primary infection, and declined rapidly during the first year after infection.
Conflict of interest statement
Figures
Comment in
-
Shedding Patterns of Genital Herpes Simplex Virus Infections.JAMA. 2022 Nov 1;328(17):1710-1711. doi: 10.1001/jama.2022.18930. JAMA. 2022. PMID: 36272101 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
