

Multiple cerebral infarctions due to calcified amorphous tumor growing rapidly from an antecedent infection and decreasing rapidly by detachment of fibrin and antithrombotic drugs: a case report
- PMID: 36273125
- PMCID: PMC9587607
- DOI: 10.1186/s12883-022-02918-5
Multiple cerebral infarctions due to calcified amorphous tumor growing rapidly from an antecedent infection and decreasing rapidly by detachment of fibrin and antithrombotic drugs: a case report
Abstract
Background: Calcified amorphous tumor (CAT) of the heart is a rare non-neoplastic intracardiac mass, a calcium deposition surrounded by amorphous fibrous tissue, and possibly causes cerebral embolism. Even rarer is CAT associated with infection, and no CAT with antecedent infection has been reported to our knowledge. In addition, although some CAT in patients on hemodialysis has been reported to grow rapidly, no case has been reported on CAT that grew and diminished rapidly in a short period of time. Here, we report the case of an 82-year-old Japanese woman with normal renal function who developed multiple cerebral infarctions due to CAT that grew rapidly, associated with inflammation from an antecedent infection, and diminished rapidly by detachment of fibrin on the mass surface and antithrombotic drugs.
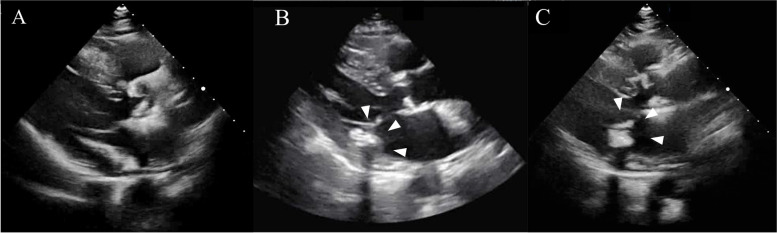
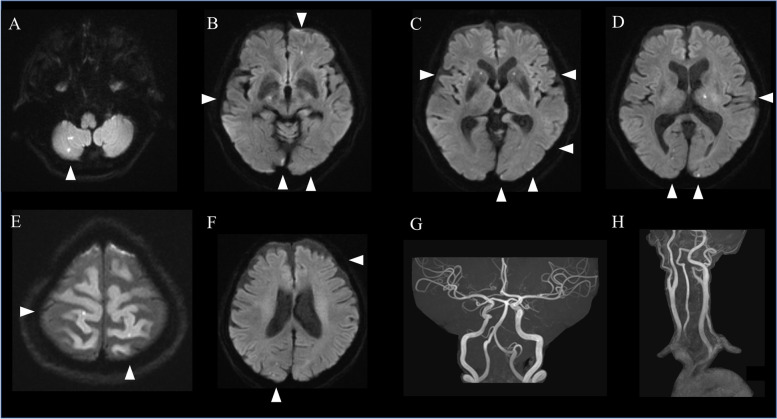
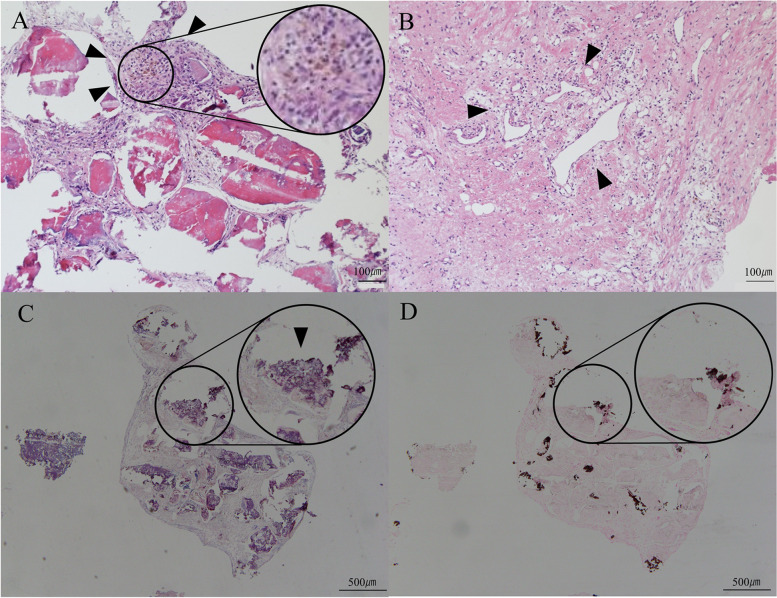
Case presentation: The patient developed fever after dental treatment and found musical hallucination on the left ear worsened in degree and frequency. In a nearby clinic, she was treated with antibiotics, and her body temperature turned to normal in approximately 1 month. She presented to our hospital for workup on the worsened musical hallucination. Magnetic resonance imaging (MRI) showed multiple cerebral infarctions, and transthoracic echocardiography (TTE) revealed an immobile hyperechoic mass with an acoustic shadow arising from a posterior cusp of the mitral valve. CAT was suspected and treated with apixaban and aspirin. Follow-up MRI and TTE showed newly developed multiple cerebral infarctions and rapidly diminished CAT. Cardiac surgery was performed to resect the CAT. The pathological findings showed calcifications surrounded by amorphous fibrous tissue including fibrin, indicating CAT. The patient's symptoms improved and no cerebral infarctions recurred in 4 months follow-up.
Conclusion: Inflammation from an antecedent infection can cause CAT to grow rapidly. Fibrous tissue including fibrin may attach to the surface of CAT, resulting in multiple cerebral infarctions. Fibrous tissue may detach and disappear by antithrombotic drugs, leading to a rapid diminishment of CAT in size.
Keywords: Antecedent infection; Calcified amorphous tumor; Case report; Fibrin; Multiple cerebral infarctions.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no known conflict of interest or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
