

A 60-Year-Old Woman with Primary Biliary Cholangitis and Crohn's Ileitis Following the Suspension of Ursodeoxycholic Acid
- PMID: 36273261
- PMCID: PMC9608254
- DOI: 10.12659/AJCR.936387
A 60-Year-Old Woman with Primary Biliary Cholangitis and Crohn's Ileitis Following the Suspension of Ursodeoxycholic Acid
Abstract
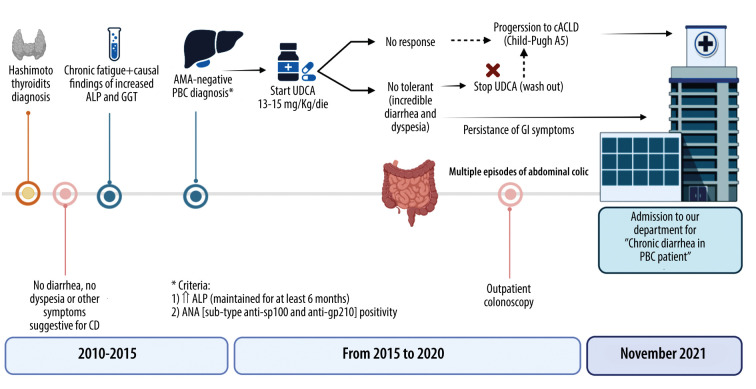
BACKGROUND There is a recognized association between inflammatory bowel disease (IBD) and hepatobiliary autoimmune disease, particularly primary sclerosing cholangitis (PSC). There have been fewer reported cases of IBD and primary biliary cholangitis (PBC), which is treated with ursodeoxycholic acid (UDCA). This report presents the case of a 60-year-old woman with PBC who was diagnosed with Crohn's ileitis after suspension of UDCA treatment. CASE REPORT A 66-year-old female patient with PBC was admitted to our department for irrepressible chronic diarrhea and recurrent abdominal pain. PBC was diagnosed on the basis of serological data: chronic (>6 months) increase in alkaline phosphatase (ALP) associated with positivity for specific anti-nuclear antibodies (sp100 and gp210), without requiring a liver biopsy and a magnetic resonance cholangiopancreatography to rule out PSC. Given the intolerance and non-responsiveness according to the Toronto criteria (ALP <1.67 times the normal limit after 2 years) to UDCA at 15 mg/kg/day, an oral monotherapy treatment using obeticholic acid at 5 mg/day was prescribed. The patient complained of abdominal pain and upper gastrointestinal symptoms. The endoscopic/histologic and radiologic examinations supported the diagnosis of Crohn's ileitis. Given the potential benefits to PBC patients of what is described as off-label therapy, budesonide at a dosage of 9 mg/day p.o. was also administered. One month after discharge, an improvement was observed both in the cholestasis indices and in gastrointestinal symptoms. CONCLUSIONS This report presents a case of PBC in which the patient was diagnosed with Crohn's ileitis after cessation of treatment with UDCA, and highlights the importance of recognizing the association between autoimmune hepatobiliary disease and IBD.
Conflict of interest statement
Figures


References
-
- European Association for the Study of the Liver EASL Clinical Practice Guidelines: The diagnosis and management of patients with primary biliary cholangitis. J Hepatol. 2017;67(1):145–72. - PubMed
-
- Younossi ZM, Bernstein D, Shiffman ML, et al. Diagnosis and management of primary biliary cholangitis. Am J Gastroenterol. 2019;114(1):48–63. - PubMed
-
- Khoshpouri P, Habibabadi RR, Hazhirkarzar B, et al. Imaging features of primary sclerosing cholangitis: From diagnosis to liver transplant follow-up. Radiographics. 2019;39(7):1938–64. - PubMed
-
- Goet JC, Murillo Perez CF, Harms MH, et al. A Comparison of prognostic scores (Mayo, UK-PBC, and GLOBE) in primary biliary cholangitis. Am J Gastroenterol. 2021;116(7):1514–22. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
